Implantable cardioverter-defibrillators (ICDs)
Overview
An implantable cardioverter-defibrillator (ICD) controls your heart rhythm by delivering shocks to your heart when it detects an abnormal heartbeat.
An implantable cardioverter-defibrillator (ICD) is a small battery-powered device placed in your chest to detect and stop abnormal heartbeats (arrhythmias). An ICD continuously monitors your heartbeat and delivers electric shocks, when needed, to restore a normal heart rhythm.
You might need an ICD if you have a dangerously fast heartbeat that keeps your heart from supplying enough blood to the rest of your body (such as ventricular tachycardia or ventricular fibrillation) or if you are at high risk of such a heart rhythm problem (arrhythmia), usually because of a weak heart muscle.
An ICD differs from a pacemaker — an implantable device that can prevent dangerously slow heartbeats.
Types
An ICD is a type of cardiac therapy device. There are two basic types:
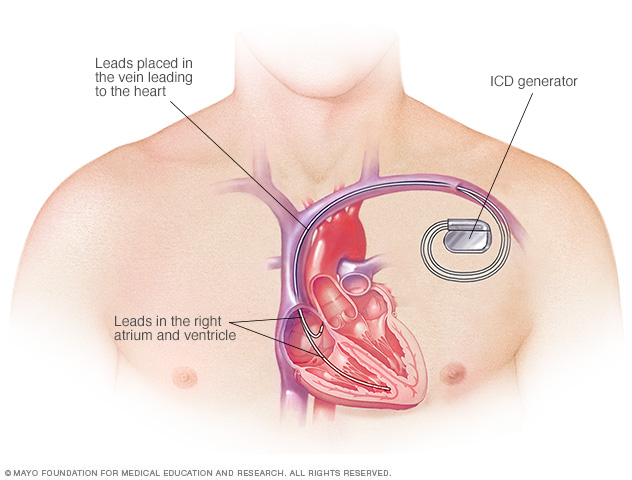
- A traditional ICD is implanted in your chest, and the wires (leads) attach to your heart. The implant procedure requires invasive surgery.
- A subcutaneous ICD (S-ICD) is another option that's implanted under the skin at the side of the chest below the armpit. It's attached to an electrode that runs along your breastbone. An S-ICD is larger than a traditional ICD but doesn't attach to your heart.
Why it's done
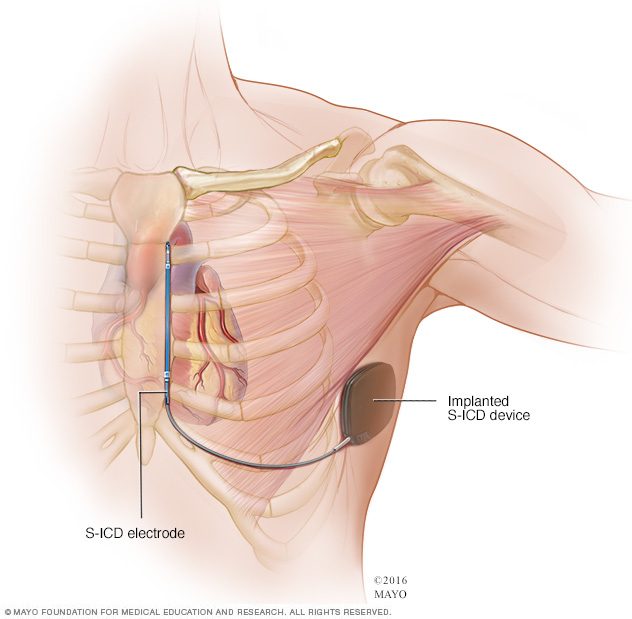
A subcutaneous implantable cardioverter-defibrillator (S-ICD) is a less invasive alternative to a traditional ICD. Your doctor implants the S-ICD device under the skin at the side of the chest below the armpit and connects it to an electrode that runs along the breastbone.
An ICD constantly monitors for abnormal heartbeats and instantly tries to correct them. It helps when your heart stops beating effectively (cardiac arrest), even when you're not near a hospital.
Your doctor may recommend an ICD if you've had signs or symptoms of certain abnormal heartbeats called sustained ventricular tachycardia, including fainting. It might also be recommended if you survived a cardiac arrest. Other reasons you may benefit from an ICD are:
- A history of coronary artery disease and heart attack that has weakened your heart
- An enlarged heart muscle
- A genetic heart condition that increases your risk of dangerously fast heart rhythms, such as some types of long QT syndrome
- Other rare conditions that may affect your heartbeat
Your doctor may recommend an S-ICD if you have structural defects in your heart that prevent attaching wires to the heart through your blood vessels, or if you want to avoid a traditional ICD.
Risks
Possible risks of having an ICD implanted include:
- Infection at the implant site
- Swelling, bleeding or bruising
- Blood vessel damage from ICD leads
- Bleeding around your heart, which can be life-threatening
- Blood leaking through the heart valve (regurgitation) where the ICD lead is placed
- Collapsed lung (pneumothorax)
How you prepare
Before you get an ICD, your doctor will order several tests, which may include:
- Electrocardiography (ECG or EKG). An ECG is a quick and painless test that measures the electrical signals that make your heart beat. Sticky patches (electrodes) are placed on your chest and sometimes your arms and legs. Wires connect the electrodes to a computer, which displays the test results. An ECG can show if your heart is beating too fast, too slow or not at all.
- Echocardiography. This noninvasive test uses sound waves to create pictures of your heart in motion. It shows your doctor the size and structure of your heart and how blood is flowing through your heart.
-
Holter monitoring. A Holter monitor is a small, wearable device that keeps track of your heart rhythm. It may be able to spot occasionally abnormal heart rhythms that an ECG missed. Your doctor may want you to wear a Holter monitor for 1 to 2 days. Wires from electrodes on your chest go to a battery-operated recording device carried in your pocket or worn on a belt or shoulder strap.
While wearing the monitor, you'll keep a diary of your activities and symptoms. Your doctor will compare the diary with the electrical recordings and try to figure out the cause of your symptoms.
- Event recorder. If you didn't have any irregular heart rhythms while you wore a Holter monitor, your doctor may recommend an event recorder, which can be worn for a longer time. There are several different types of event recorders. Event recorders are similar to Holter monitors and generally require you to push a button when you feel symptoms.
- Electrophysiology study (EP study). The doctor guides a flexible tube (catheter) through a blood vessel into your heart. More than one catheter is often used. Sensors on the tip of each catheter send signals and record your heart's electricity. Your doctor uses this information to identify the area that is causing your abnormal heartbeat.
What you can expect
Before the procedure
If you're having an ICD implanted, you'll likely be asked to avoid food and drinks for at least 8 hours before the procedure.
Talk to your doctor about any medications you take and whether you should continue to take them before the procedure to implant an ICD.
During the procedure
A specialist will insert an IV into your forearm or hand and give you a medication called a sedative to help you relax.
You will be given general anesthesia (fully asleep).
During surgery, the doctor guides one or more flexible, insulated wires (leads) into veins near your collarbone to your heart using X-ray images as a guide. The ends of the leads attach to your heart. The other ends attach to a device (shock generator) that's implanted under the skin beneath your collarbone. The procedure usually takes a few hours.
Once the ICD is in place, your doctor will test it and program it for your specific heart rhythm needs. Testing the ICD might require speeding up your heart and then shocking it back into a normal rhythm.
Depending on the problem with your heartbeat, your ICD could be programmed for:
- Low-energy pacing. You may feel nothing or a painless fluttering in your chest when your ICD responds to mild changes in your heartbeat.
- A higher energy shock. For more-serious heart rhythm problems, the ICD may deliver a higher energy shock. This shock can be painful, possibly making you feel as if you've been kicked in the chest. The pain usually lasts only a second, and there shouldn't be discomfort after the shock ends.
Usually, only one shock is needed to restore a normal heartbeat. Sometimes you might have two or more shocks during a 24-hour period.
Having three or more shocks in a short amount of time is called an electrical or arrhythmia storm. If you have an electrical storm, you should call 911 or seek emergency medical help to see if your ICD is working properly or if you're having abnormal heartbeats.
If necessary, the ICD can be adjusted to reduce the number and frequency of shocks. You may need medications to make your heart beat regularly and decrease your risk of an ICD electrical storm.
After the procedure
You'll usually be released on the day after your procedure. You'll need to arrange to have someone to drive you home and help you while you are recovering.
The area where the ICD is implanted can be swollen and tender for a few days or weeks. Your doctor might prescribe pain medication. Aspirin and ibuprofen aren't recommended because they may increase your risk of bleeding.
You'll need to avoid abrupt movements that raise your left arm above your shoulder for up to eight weeks so the leads don't move until the area has healed. You may need to limit your driving, depending the type of ICD received. Your doctor will give you instructions on when it's safe to return to driving and other daily activities.
For about four weeks after surgery, your doctor might ask you to avoid:
- Vigorous, above-the-shoulder activities or exercises, including golf, tennis, swimming, bicycling, bowling or vacuuming
- Heavy lifting
- Strenuous exercise programs
Your doctor will probably tell you to avoid contact sports indefinitely. Heavy contact may damage your device or dislodge the wires.
Long-term precautions
Problems with your ICD due to electrical signals (electrical interference) are rare. Still, take precautions with the following:
- Cellular phones and other mobile devices. It's safe to talk on a cellphone, but avoid placing your cellphone within 6 inches (about 15 centimeters) of your ICD site when the phone is turned on. Although unlikely, your ICD could mistake a cellphone's signal for a heartbeat and slow your heartbeat, causing symptoms such as sudden fatigue.
-
Security systems. After surgery, you'll receive a card that says you have an ICD. Show your card to airport personnel because the ICD may set off airport security alarms.
Also, hand-held metal detectors often contain a magnet that can interfere with your ICD. Limit scanning with a hand-held detector to less than 30 seconds over the site of your ICD or make a request for a manual search.
- Medical equipment. Tell doctors, medical technicians and dentists that you have an ICD. Some procedures, such as magnetic resonance imaging (MRI), magnetic resonance angiography (MRA), and radiofrequency or microwave ablation may not be recommended if you have an ICD. Your doctor can tell you if you need an alternative test.
- Power generators. Stand at least 2 feet (0.6 meters) from welding equipment, high-voltage transformers or motor-generator systems. If you work around such equipment, your doctor can arrange a test in your workplace to see if the equipment affects your ICD.
- Headphones and wireless chargers. Headphones may contain a magnetic substance that can interfere with your ICD. Keep headphones and wireless chargers at least 6 inches (about 15 centimeters) from your ICD.
- Magnets. These might affect your ICD, so it's a good idea to keep magnets at least 6 inches (15 centimeters) from your ICD site.
Devices that pose little or no risk to your ICD include microwave ovens, televisions and remote controls, AM/FM radios, toasters, electric blankets, electric shavers and electric drills, computers, scanners, printers, and GPS devices.
Driving restrictions
If you have an ICD to treat ventricular arrhythmia, driving a vehicle may pose risks to yourself and others. The combination of arrhythmia and shocks from your ICD can cause fainting, which would be dangerous while you're driving.
Many countries have driving restrictions for people with ICDs. If your ICD was implanted due to a previous cardiac arrest or ventricular arrhythmia, your doctor may recommend waiting several months before driving or operating a vehicle. If you have a shock, with or without fainting, tell your doctor and follow his or her recommendations. In most cases, you'll be discouraged from driving until you've been shock-free for several months.
If you have an ICD but have no history of life-threatening arrhythmias, you can usually resume driving about a week after your procedure if you've had no shocks. Discuss your situation with your doctor.
You usually can't get a commercial driver's license if you have an ICD.
Results
ICDs are the main treatment for anyone who has survived cardiac arrest, and they're increasingly used in people at high risk of sudden cardiac arrest. An ICD lowers your risk of sudden death from cardiac arrest more than medication alone.
Although the electrical shocks can be unsettling, they're a sign that the ICD is effectively treating your heart rhythm problem and protecting you from sudden death. Talk to your doctor about how to best care for your ICD.
The lithium battery in your ICD can last 5 to 7 years. The battery will be checked during your regular checkups, which should occur about every six months. When the battery is nearly out of power, the generator is replaced with a new one during a minor outpatient procedure.
ICDs and end-of-life issues
If you have an ICD and become terminally ill, your ICD will still deliver shocks if it isn't deactivated. Your doctor can perform a simple procedure to turn off your ICD, if desired. Turning off the device can prevent unwanted shocks and unnecessary suffering. Doing so won't immediately cause your heart to stop.
Talk to your doctor about your wishes. Also talk to family members or the person designated to make medical decisions for you about what you'd like to do in an end-of-life care situation.
Content Last Updated: August 27, 2021
Content provided by Mayo Clinic ©1998-2026 Mayo Foundation for Medical Education and Research (MFMER). All rights reserved. Terms of Use