Infant reflux
Overview
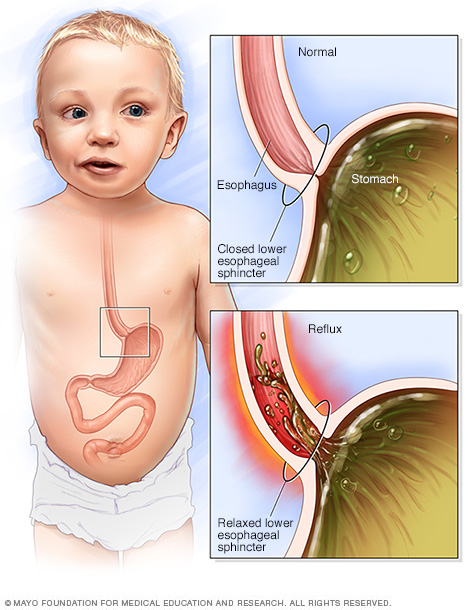
If the muscle between the esophagus and the stomach (lower esophageal sphincter) relaxes when the stomach is full, food might flow up the baby’s esophagus.
Infant reflux, when a baby spits up, occurs when food moves back up from a baby’s stomach. Reflux occurs in healthy infants multiple times a day. As long as your baby is healthy, content and growing well, reflux is not a cause for concern.
Sometimes called gastroesophageal reflux (GER), the condition is rarely serious and becomes less common as a baby gets older. It’s unusual for infant reflux to continue after age 18 months.
Rarely, infant reflux can be accompanied by worrisome symptoms, such as failure to thrive or weight loss. These can indicate a medical problem, such as an allergy, a blockage in the digestive system or gastroesophageal reflux disease (GERD).
Symptoms
Infant reflux generally isn’t a cause for concern. It’s unusual for the stomach contents to have enough acid to irritate the throat or esophagus and to cause signs and symptoms.
When to see a doctor
See your baby’s doctor if your baby:
- Isn’t gaining weight
- Consistently spits up forcefully, causing stomach contents to shoot out of his or her mouth (projectile vomiting)
- Spits up green or yellow fluid
- Spits up blood or a material that looks like coffee grounds
- Refuses food
- Has blood in his or her stool
- Has difficulty breathing or a chronic cough
- Begins spitting up at age 6 months or older
- Is unusually irritable after eating
Some of these signs can indicate possibly serious but treatable conditions, such as GERD or a blockage in the digestive tract.
Causes
In infants, the ring of muscle between the esophagus and the stomach — the lower esophageal sphincter (LES) — is not yet fully mature. That allows stomach contents to flow back up. Eventually, the LES will open only when your baby swallows and will remain tightly closed at other times, keeping stomach contents where they belong.
The factors that contribute to infant reflux are common in babies and often can’t be avoided. These factors include:
- Lying flat most of the time
- Consuming an almost completely liquid diet
- Being born prematurely
Occasionally, infant reflux can be caused by more-serious conditions, such as:
- GERD. The reflux has enough acid to irritate and damage the lining of the esophagus.
- Pyloric stenosis. A valve between the stomach and the small intestine is narrowed, preventing stomach contents from emptying into the small intestine.
- Food intolerance. A protein in cow’s milk is the most common trigger.
- Eosinophilic esophagitis. A certain type of white blood cell (eosinophil) builds up and injures the lining of the esophagus.
- Sandifer syndrome. This causes abnormal tilting and rotation of the head and movements that resemble seizures. It’s a rarely seen consequence of GERD.
Complications
Infant reflux usually resolves without causing problems for your baby.
If your baby has a more-serious condition such as GERD, he or she might grow poorly. Some research indicates that babies who have frequent episodes of spitting up might be more likely to develop GERD during later childhood.
Diagnosis
Your doctor will start with a physical exam and questions about your baby’s symptoms. If your baby is healthy, growing as expected and seems content, then testing usually isn’t needed. In some cases, however, your doctor might recommend:
- Ultrasound. This imaging test can detect pyloric stenosis.
- Lab tests. Blood and urine tests can help identify or rule out possible causes of recurring vomiting and poor weight gain.
- Esophageal pH monitoring. To measure the acidity in your baby’s esophagus, the doctor will insert a thin tube through the baby’s nose or mouth and into the esophagus. The tube is attached to a device that monitors acidity. Your baby might need to stay in the hospital while being monitored.
- X-rays. These images can detect abnormalities in the digestive tract, such as an obstruction. Your baby may be given a contrast liquid (barium) from a bottle before the test.
- Upper endoscopy. A special tube equipped with a camera lens and light (endoscope) is passed through your baby’s mouth and into the esophagus, stomach and first part of the small intestine. Tissue samples may be taken for analysis. For infants and children, endoscopy is usually done under general anesthesia.
Treatment
For most babies, making some adjustments to feeding will ease infant reflux until it resolves on its own.
Medications
Reflux medications aren’t recommended for children with uncomplicated reflux. However, a short-term trial of an acid-blocking medication — such as cimetidine (Tagamet HB) or famotidine (Pepcid AC) for infants ages 1 month to 1 year or omeprazole magnesium (Prilosec) for children age 1 year or older — might be recommended if your baby:
- Has poor weight gain and more-conservative treatments haven’t worked
- Refuses to feed
- Has evidence of an inflamed esophagus
- Has chronic asthma and reflux
Surgery
Rarely, the lower esophageal sphincter is surgically tightened to prevent acid from flowing back into the esophagus. This procedure is usually done only when reflux is severe enough to prevent growth or to interfere with your baby’s breathing.
Lifestyle and home remedies
To minimize reflux:
- Feed your baby in an upright position. Also hold your baby in a sitting position for 30 minutes after feeding, if possible. Gravity can help stomach contents stay where they belong. Be careful not to jostle or jiggle your baby while the food is settling.
- Try smaller, more-frequent feedings. Feed your baby slightly less than usual if you’re bottle-feeding, or cut back a little on nursing time.
- Take time to burp your baby. Frequent burps during and after feeding can keep air from building up in your baby’s stomach.
- Put baby to sleep on his or her back. Most babies should be placed on their backs to sleep, even if they have reflux.
Remember, infant reflux is usually little cause for concern. Just keep plenty of burp cloths handy as you ride it out.
Preparing for an appointment
If reflux continues after your child’s first birthday, or if your child is having symptoms such as lack of weight gain and breathing problems, you might be referred to a doctor who specializes in children’s digestive diseases (pediatric gastroenterologist).
What you can do
- Write down your baby’s symptoms, including how frequently your baby spits up and the amount of liquid that is spit up.
- Write down key medical information, including how often you feed your baby, how long the feedings last and the brand of any formula that you are using.
- Write down questions to ask your doctor.
Questions to ask your doctor
- What’s the most likely cause of my baby’s symptoms?
- Does my baby need any tests?
- What treatments are available?
- Should I make any changes in how or what I feed my baby?
Don’t hesitate to ask other questions.
What to expect from your doctor
Your doctor is likely to ask you questions, including:
- When did your baby’s symptoms start?
- Does your baby spit up with every feeding or only occasionally?
- Is your baby content between feedings?
- Have you recently switched from breastfeeding to bottle-feeding? Or have you switched infant formulas?
- How often do you feed your baby, and how much does your baby eat at each feeding?
- If you have different caregivers, does everyone feed the baby the same way each time?
- Does anything seem to improve or worsen your baby’s symptoms?
Content Last Updated: December 17, 2020
Content provided by Mayo Clinic ©1998-2022 Mayo Foundation for Medical Education and Research (MFMER). All rights reserved. Terms of Use