Pulmonary atresia
Overview
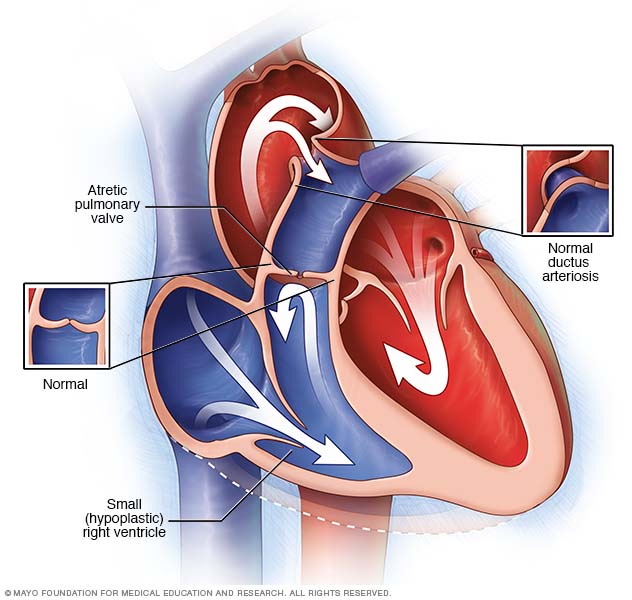
In pulmonary atresia, the valve that lets blood flow from the heart to the lungs isn't formed properly. Instead, some blood may reach the lungs via a temporary connection (ductus arteriosus) between a baby's aorta and the pulmonary artery. Some babies born with pulmonary atresia may have a small (hypoplastic) right ventricle.
Pulmonary atresia (uh-TREE-zhuh) is a heart defect present at birth (congenital) that's normally diagnosed soon after birth. In pulmonary atresia, the valve that lets blood out of the heart to go to your or your baby's lungs (pulmonary valve) doesn't form correctly.
Without a connection from the pumping chamber to the pulmonary artery, blood can't travel its normal route to pick up oxygen from the lungs. Instead, some blood travels to the lungs through other natural passages within the heart and its arteries.
These passages are necessary when your baby is developing in the womb and they normally close soon after birth. Babies with pulmonary atresia typically have a bluish cast to their skin because they aren't getting enough oxygen.
Pulmonary atresia is a life-threatening situation. Procedures to correct your baby's heart condition and medications to help your baby's heart work more effectively are the first steps to treat pulmonary atresia.
Symptoms
If your baby is born with pulmonary atresia, symptoms will be noticeable soon after birth. Your baby's signs and symptoms may include:
- Blue- or gray-toned skin (cyanosis)
- Fast breathing or shortness of breath
- Easily tiring or being fatigued
- Feeding problems
When to see a doctor
Your baby will most likely be diagnosed with pulmonary atresia soon after birth. However, if your baby has any symptoms of pulmonary atresia after you've returned home, seek emergency medical attention.
Causes
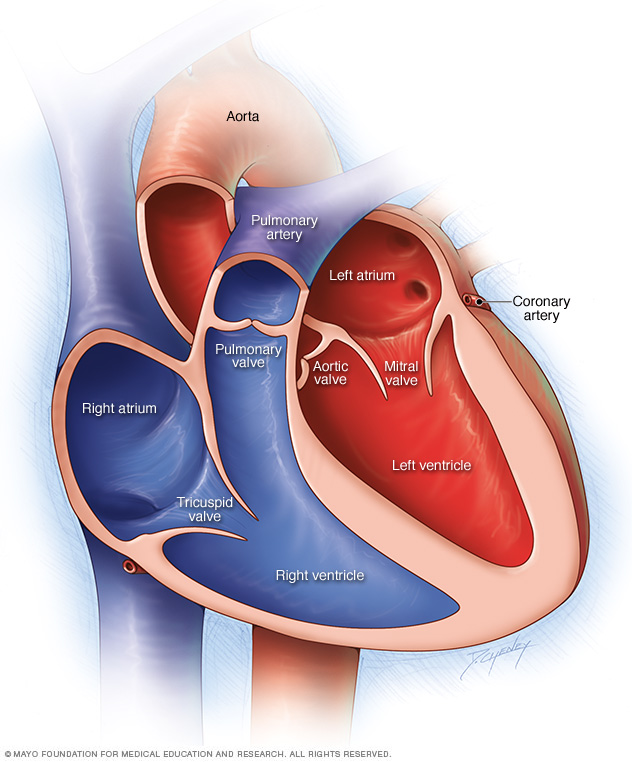
A typical heart has two upper and two lower chambers. The upper chambers — the right and left atria — receive incoming blood. The lower chambers — the right and left ventricles — pump blood out of your heart. The heart valves, which keep blood flowing in the right direction, are gates at the chamber openings (for the tricuspid and mitral valves) and exits (for the pulmonary and aortic valves).
There's no known cause of pulmonary atresia. To understand the problems pulmonary atresia causes, it's helpful to know how the heart works.
How the heart works
The heart is divided into four hollow chambers, two on the right and two on the left. In performing its basic job — pumping blood throughout the body — the heart uses its left and right sides for different tasks.
The right side of the heart moves blood to the lungs through vessels called pulmonary arteries. In the lungs, blood picks up oxygen then returns to the heart's left side through the pulmonary veins. The left side of the heart then pumps the blood through the aorta and out to the rest of the body to supply your baby's body with oxygen.
Blood moves through your baby's heart in one direction through valves that open and close as the heart beats. The valve that allows blood out of your baby's heart and into the lungs to pick up oxygen is called the pulmonary valve.
In pulmonary atresia, the pulmonary valve doesn't develop properly, preventing it from opening. Blood can't flow from the right ventricle to the lungs.
Before birth, the improperly formed valve isn't life-threatening, because the placenta provides oxygen for your baby instead of the lungs. Blood entering the right side of your baby's heart passes through a hole (foramen ovale) between the top chambers of your baby's heart, so the oxygen-rich blood can be pumped out to the rest of your baby's body through the aorta.
After birth, your baby's lungs must provide oxygen for his or her body. In pulmonary atresia, without a working pulmonary valve, blood must find another route to reach your baby's lungs.
The foramen ovale usually shuts soon after birth, but may stay open in pulmonary atresia. Newborn babies also have a temporary connection (ductus arteriosus) between the aorta and the pulmonary artery.
This passage allows some of the oxygen-poor blood to travel to the lungs where it can pick up oxygen to supply your baby's body. The ductus arteriosus normally closes soon after birth, but can be kept open with medications.
In some cases, there may be a second hole in the tissue that separates the main pumping chambers of your baby's heart, called a ventricular septal defect (VSD).
The VSD allows a pathway for blood to pass through the right ventricle into the left ventricle. Children with pulmonary atresia and a VSD often have additional abnormalities of the lungs and the arteries that bring blood to the lungs.
If there's no VSD, the right ventricle receives little blood flow before birth and often doesn't develop fully. This is a condition called pulmonary atresia with intact ventricular septum (PA/IVS).
Risk factors
In most cases, the exact cause of a congenital heart defect, such as pulmonary atresia, is unknown. However, several factors may increase the risk of a baby being born with a congenital heart defect, including:
- A parent or sibling with a congenital heart defect
- A mother who is obese before getting pregnant
- Smoking before or during pregnancy
- A mother who has poorly controlled diabetes
- Use of some types of medications during pregnancy, such as certain acne drugs and blood pressure medications
Complications
Without treatment, pulmonary atresia is nearly always fatal. Even after surgical repairs, you'll need to carefully monitor your child's health for any changes that could signal a problem.
People with structural heart problems, such as pulmonary atresia, are at a higher risk of infectious endocarditis than the general population. Infectious endocarditis is an inflammation of the valves and inner lining of the heart caused by a bacterial infection.
Even after treatment, people born with pulmonary atresia appear to face a higher risk of certain heart problems, such as abnormal heart rhythms (arrhythmias) and heart failure as adults.
Prevention
Because the exact cause of pulmonary atresia is unknown, it may not be possible to prevent it. However, there are some things you can do that might reduce your child's overall risk of congenital heart defects, such as:
- Control chronic medical conditions. If you have diabetes, keeping your blood sugar in check can reduce the risk of heart defects. If you have other chronic conditions, such as high blood pressure or epilepsy, that require the use of medications, discuss the risks and benefits of these drugs with your doctor.
- Don't smoke. Smoking cigarettes during pregnancy may increase the risk of heart defects in your baby.
- Maintain a healthy weight. If you're obese, you have a higher risk of having a baby with a congenital heart defect.
- Get a German measles (rubella) vaccine. If you develop German measles during pregnancy, it may affect your baby's heart development. Being vaccinated before you try to conceive likely eliminates this risk. However, no link has been shown between rubella and the development of pulmonary atresia.
Diagnosis
Tests to diagnose pulmonary atresia may include:
- Pulse oximetry. This noninvasive test measures the oxygen levels in the blood through a small, clamp-like device that's placed on a finger, earlobe or toe.
- X-ray. An X-ray shows the size and shape of your child's internal tissues, bones and organs. This can help your baby's doctor see the extent of your baby's pulmonary atresia.
- Electrocardiogram (ECG). In this test, sensor patches with wires attached (electrodes) measure the electrical impulses given off by your child's heart. This test detects any abnormal heart rhythms (arrhythmias or dysrhythmias) and may show heart muscle stress.
- Echocardiogram. In an echocardiogram, sound waves create detailed images of your child's heart. Your child's doctor usually uses an echocardiogram to diagnose pulmonary atresia. Your doctor may diagnose your baby's pulmonary atresia through an echocardiogram of your abdomen before you deliver your baby (fetal echocardiogram).
- Cardiac catheterization. In this test, your child's doctor inserts a thin, flexible tube (catheter) into a blood vessel in your child's groin and guides it to your child's heart using X-ray imaging. This test provides detailed information about your child's heart structure and the blood pressure and oxygen levels in your child's heart, pulmonary artery and aorta. Your child's doctor may inject a special dye into the catheter to make the arteries visible under X-ray.
- CT scan. A CT scan of the chest shows the structure of the heart and the position of the pulmonary artery.
Treatment
Your baby will need urgent medical attention once pulmonary atresia symptoms develop. The choice of surgeries or procedures depends on the severity of your child's condition.
Medications
An intravenous drug called prostaglandin will prevent closure of the natural connection (ductus arteriosus) between the pulmonary artery and the aorta. This is not a permanent solution, but it gives your doctors additional time to determine what type of surgery or procedure might be best for your child.
Procedures via catheterization
In some cases, repairs can be made via a long, thin tube (catheter) inserted into a large vein in your baby's groin and threaded up to the heart. These procedures include:
- Balloon atrial septostomy. A balloon can also be used to enlarge the natural hole (foramen ovale) in the wall between the upper two chambers of the heart. This hole usually closes shortly after birth. Enlarging it increases the amount of blood available to travel to the lungs.
- Stent placement. Your baby's doctor may place a rigid tube (stent) in the natural connection between the aorta and pulmonary artery (ductus arteriosus). This opening also usually closes soon after birth. Keeping it open allows blood to travel to the lungs.
Heart surgery
The type of surgical repair needed will depend on the size of your child's right ventricle and pulmonary artery. Babies with pulmonary atresia often require a series of heart operations over time. Some examples include:
- Shunting. Creating a bypass (shunt) from the main blood vessel leading out of the heart (aorta) to the pulmonary arteries allows for adequate blood flow to the lungs. However, babies usually outgrow this shunt within a few months.
- Glenn procedure. In this surgery, one of the large veins that normally returns blood to the heart is connected directly to the pulmonary artery instead. Another large vein continues to provide blood to the right side of the heart, which pumps it through the surgically repaired pulmonary valve. This can help the right ventricle grow larger.
- Fontan procedure. If the right ventricle remains too small to be useful, surgeons may use a Fontan procedure to create a pathway that allows most, if not all, of the blood coming to the heart to flow directly into the pulmonary artery.
- Heart transplant. In some cases, the heart is too damaged to repair and a heart transplant may be necessary.
Potential future treatments
It's possible that pulmonary atresia might someday be treated with fetal surgery during pregnancy.
Lifestyle and home remedies
Here are some tips for caring for your child after coming home from the hospital:
- Keep regular follow-up appointments with your child's doctor. Your child will likely need regular appointments with a doctor trained in congenital heart conditions. These appointments need to continue even after your child is an adult. Ask your child's doctor how frequently your child needs to be seen.
- Help your child stay active. Encourage as much normal play and activity as your child is able to tolerate, with ample opportunity for rest and nap time. Staying active helps your child's heart stay fit. As your child grows, talk with the cardiologist about which activities are best for your child. If some are off-limits, such as competitive sports, encourage your child in other pursuits rather than focusing on what he or she can't do.
- Keep up with routine well-child care. Standard vaccinations are encouraged for children with congenital heart defects, as well as vaccines against the flu, pneumonia and respiratory syncytial virus infections.
- Preventive antibiotics. Your child's cardiologist may recommend that your child take preventive antibiotics before certain dental and other procedures to prevent bacteria from entering the bloodstream and infecting the inner lining of the heart (infective endocarditis). Practicing good oral hygiene — brushing and flossing teeth, getting regular dental checkups — is another good way of preventing infection.
Coping and support
It's natural for many parents to feel worried about their child's health, even after treatment of a congenital heart defect. Although many children who have congenital heart defects can do the same things children without heart defects can, here are a few things to keep in mind if your child has a congenital heart defect:
- Developmental difficulties. Because some children who have congenital heart defects may have had a long recovery time from surgeries or procedures, they may developmentally lag behind other children their age. Talk to your child's doctor about ways to help your child through his or her developmental difficulties.
- Emotional difficulties. Many children who have developmental difficulties may feel insecure about their abilities and may have emotional difficulties as they reach school age. Talk to your child's doctor about ways you can help your child cope with these problems, which may include support groups for parents, or a visit to a therapist or psychologist for your child.
- Support groups. Having a child with a serious medical problem isn't easy and, depending on the severity of the defect, may be very difficult and frightening. You may find that talking with other parents who've been through the same situation brings you comfort and encouragement. Ask your child's doctor if there are any local support groups.
Preparing for an appointment
It's most likely that your child would be diagnosed with pulmonary atresia soon after birth while still in the hospital. If your child is diagnosed with pulmonary atresia, you'll be referred to a heart specialist (cardiologist) for ongoing care.
Here's some information to help you get ready for your appointment.
What you can do
When you make the appointment, ask if there's anything you need to do in advance, such as fill out forms or restrict your child's diet. For some imaging tests, for example, your child might need to fast for a time beforehand.
Take a family member or friend to the appointment, if possible. Someone who accompanies you can help you remember the information you're given.
Make a list of:
- Your child's symptoms, including any that seem unrelated to pulmonary atresia, and when they began.
- Key personal information, including a family history of heart defects, pulmonary hypertension, lung disease, heart disease, stroke, high blood pressure or diabetes.
- All medications, vitamins or supplements that your child takes, including doses. Also, tell your doctor if you've recently stopped taking any medications, or if you took medications during pregnancy.
- Questions to ask your child's doctor.
Some basic questions to ask your doctor about pulmonary atresia include:
- What tests will my child need?
- What's the best treatment?
- Are there activities my child should avoid as he or she grows?
- How often should my child be screened for changes in his or her condition?
- Are there brochures or other printed materials I can have? What websites do you recommend?
Don't hesitate to ask any questions you have.
What to expect from your child's doctor
Your doctor is likely to ask you questions, including:
- Has anyone else in your family been diagnosed with pulmonary atresia or another heart defect?
- Have your child's symptoms been continuous or occasional?
- How severe are your child's symptoms?
- What, if anything, seems to improve your child's symptoms?
- What, if anything, appears to worsen your child's symptoms?
Content Last Updated: June 29, 2021
Content provided by Mayo Clinic ©1998-2026 Mayo Foundation for Medical Education and Research (MFMER). All rights reserved. Terms of Use