Bronchiolitis
Overview
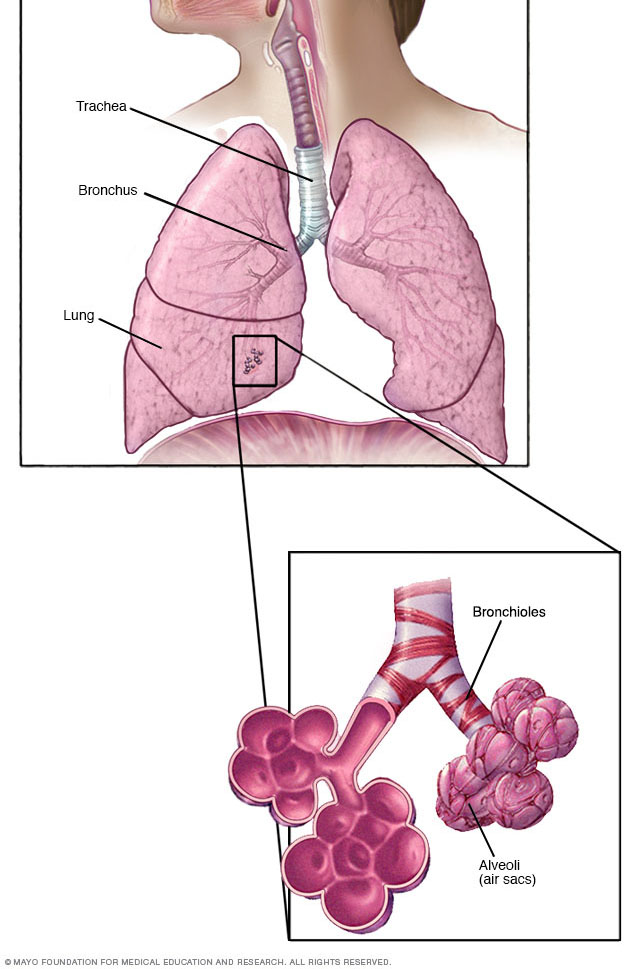
In your lungs, the main airways (bronchi) branch off into smaller and smaller passageways — the smallest, called bronchioles, lead to tiny air sacs (alveoli).
Bronchiolitis is a common lung infection in young children and infants. It causes inflammation and congestion in the small airways (bronchioles) of the lung. Bronchiolitis is almost always caused by a virus. Typically, the peak time for bronchiolitis is during the winter months.
Bronchiolitis starts out with symptoms similar to those of a common cold, but then progresses to coughing, wheezing and sometimes difficulty breathing. Symptoms of bronchiolitis can last for several days to weeks.
Most children get better with care at home. A small percentage of children require hospitalization.
Symptoms
For the first few days, the signs and symptoms of bronchiolitis are similar to those of a cold:
- Runny nose
- Stuffy nose
- Cough
- Slight fever (not always present)
After this, there may be a week or more of difficulty breathing or a whistling noise when the child breathes out (wheezing).
Many infants also have an ear infection (otitis media).
When to see a doctor
If it's difficult to get your child to eat or drink and his or her breathing becomes more rapid or labored, call your child's doctor. This is especially important if your child is younger than 12 weeks old or has other risk factors for bronchiolitis — including premature birth or a heart or lung condition.
The following signs and symptoms are reasons to seek prompt medical attention:
- Audible wheezing sounds
- Breathing very fast — more than 60 breaths a minute (tachypnea) — and shallowly
- Labored breathing — the ribs seem to suck inward when the infant inhales
- Sluggish or lethargic appearance
- Refusal to drink enough, or breathing too fast to eat or drink
- Skin turning blue, especially the lips and fingernails (cyanosis)
Causes
Bronchiolitis occurs when a virus infects the bronchioles, which are the smallest airways in your lungs. The infection makes the bronchioles swell and become inflamed. Mucus collects in these airways, which makes it difficult for air to flow freely in and out of the lungs.
Most cases of bronchiolitis are caused by the respiratory syncytial virus (RSV). RSV is a common virus that infects just about every child by 2 years of age. Outbreaks of RSV infection occur every winter, and individuals can be reinfected, as previous infection does not appear to cause lasting immunity. Bronchiolitis also can be caused by other viruses, including those that cause the flu or the common cold.
The viruses that cause bronchiolitis are easily spread. You can contract them through droplets in the air when someone who is sick coughs, sneezes or talks. You can also get them by touching shared objects — such as utensils, towels or toys — and then touching your eyes, nose or mouth.
Risk factors
Bronchiolitis typically affects children under the age of 2 years. Infants younger than 3 months of age are at greatest risk of getting bronchiolitis because their lungs and immune systems aren't yet fully developed.
Other factors that are linked with an increased risk of bronchiolitis in infants and with more-severe cases include:
- Premature birth
- Underlying heart or lung condition
- Depressed immune system
- Exposure to tobacco smoke
- Never having been breast-fed (breast-fed babies receive immune benefits from the mother)
- Contact with multiple children, such as in a child care setting
- Spending time in crowded environments
- Having siblings who attend school or get child care services and bring home the infection
Complications
Complications of severe bronchiolitis may include:
- Blue lips or skin (cyanosis), caused by lack of oxygen
- Pauses in breathing (apnea), which is most likely to occur in premature babies and in babies within the first two months of life
- Dehydration
- Low oxygen levels and respiratory failure
If these occur, your child may need to be in the hospital. Severe respiratory failure may require that a tube be inserted into the windpipe (trachea) to help the child's breathing until the infection has run its course.
If your baby was born prematurely, has a heart or lung condition, or has a depressed immune system, watch closely for beginning signs of bronchiolitis. The infection can quickly become severe. In such cases, your child will usually need hospitalization.
Prevention
Because the viruses that cause bronchiolitis spread from person to person, one of the best ways to prevent it is to wash your hands frequently — especially before touching your baby when you have a cold or other respiratory illness. Wearing a face mask at this time is appropriate.
If your child has bronchiolitis, keep him or her at home until the illness is past to avoid spreading it to others.
Other commonsense ways to help curb infection include:
- Limit contact with people who have a fever or cold. If your child is a newborn, especially a premature newborn, avoid exposure to people with colds, especially in the first two months of life.
- Clean and disinfect surfaces. Clean and disinfect surfaces and objects that people frequently touch, such as toys and doorknobs. This is especially important if a family member is sick.
- Cover coughs and sneezes. Cover your mouth and nose with a tissue. Then throw away the tissue and wash your hands or use alcohol-based hand sanitizer.
- Use your own drinking glass. Don't share glasses with others, especially if someone in your family is ill.
- Wash hands often. Frequently wash your own hands and those of your child. Keep an alcohol-based hand sanitizer handy for yourself and your child when you're away from home.
- Breast-feed. Respiratory infections are significantly less common in breast-fed babies.
Vaccines and medications
There are no vaccines for the most common causes of bronchiolitis (RSV and rhinovirus). However, an annual flu shot is recommended for everyone older than 6 months.
Infants at high risk of the RSV infection, such as those born prematurely or with a heart or lung condition or who have a depressed immune system, may be given the medication palivizumab (Synagis) to decrease the likelihood of RSV infections.
Diagnosis
Tests and X-rays are not usually needed to diagnose bronchiolitis. The doctor can usually identify the problem by observing your child and listening to the lungs with a stethoscope.
If your child is at risk of severe bronchiolitis, if symptoms are worsening or if another problem is suspected, your doctor may order tests, including:
- Chest X-ray. Your doctor may request a chest X-ray to look for signs of pneumonia.
- Viral testing. Your doctor may collect a sample of mucus from your child to test for the virus causing bronchiolitis. This is done using a swab that's gently inserted into the nose.
- Blood tests. Occasionally, blood tests might be used to check your child's white blood cell count. An increase in white blood cells is usually a sign that the body is fighting an infection. A blood test can also determine whether the level of oxygen has decreased in your child's bloodstream.
Your doctor may also ask you about signs of dehydration, especially if your child has been refusing to drink or eat or has been vomiting. Signs of dehydration include sunken eyes, dry mouth and skin, sluggishness, and little or no urination.
Treatment
Bronchiolitis typically lasts for two to three weeks. Most children with bronchiolitis can be cared for at home with supportive care. It's important to be alert for changes in breathing difficulty, such as struggling for each breath, being unable to speak or cry because of difficulty breathing, or making grunting noises with each breath.
Because viruses cause bronchiolitis, antibiotics — which are used to treat infections caused by bacteria — aren't effective against it. Bacterial infections such as pneumonia or an ear infection can occur along with bronchiolitis, and your doctor may prescribe an antibiotic for that infection.
Drugs that open the airways (bronchodilators) haven't been found to be routinely helpful and typically aren't given for bronchiolitis. In severe cases, your doctor may elect to try a nebulized albuterol treatment to see if it helps.
Oral corticosteroid medications and pounding on the chest to loosen mucus (chest physiotherapy) have not been shown to be effective treatments for bronchiolitis and are not recommended.
Hospital care
A small percentage of children may need hospital care to manage their condition. At the hospital, a child may receive humidified oxygen to maintain sufficient oxygen in the blood, and he or she may receive fluids through a vein (intravenously) to prevent dehydration. In severe cases, a tube may be inserted into the trachea to help the child's breathing.
Lifestyle and home remedies
Although it may not be possible to shorten the length of your child's illness, you may be able to make your child more comfortable. Here are some tips to try:
- Humidify the air. If the air in your child's room is dry, a cool-mist humidifier or vaporizer can moisten the air and help ease congestion and coughing. Be sure to keep the humidifier clean to prevent the growth of bacteria and molds.
- Keep your child upright. Being in an upright position usually makes breathing easier.
- Have your child drink liquids. To prevent dehydration, give your child plenty of clear fluids to drink, such as water or juice. Your child may drink more slowly than usual, because of the congestion. Frequently offer small amounts of fluid.
- Try saline nose drops to ease congestion. You can buy these drops over-the-counter (OTC). They're effective, safe and nonirritating, even for children. To use them, put several drops into one nostril, then immediately bulb suction that nostril (but don't push the bulb too far in). Repeat the process in the other nostril.
- Consider OTC pain relievers. For treatment of fever or pain, ask your doctor about giving your child infants' or children's over-the-counter fever and pain medications such as acetaminophen (Tylenol, others) or ibuprofen (Advil, Motrin, others) as a safer alternative to aspirin. Aspirin is not recommended in children due to the risk of Reye's syndrome, a rare but potentially life-threatening condition. Children and teenagers recovering from chickenpox or flu-like symptoms should never take aspirin, as they have a higher risk of Reye's syndrome.
- Maintain a smoke-free environment. Smoke can worsen symptoms of respiratory infections. If a family member smokes, ask him or her to smoke outside of the house and outside of the car.
Don't use over-the-counter medicines, except for fever reducers and pain relievers, to treat coughs and colds in children younger than 6 years old. Also, consider avoiding use of these medicines for children younger than 12 years old.
Preparing for an appointment
You're likely to start by seeing your family doctor or your child's doctor. Here's some information to help you get ready for your appointment, and what to expect from your doctor.
What you can do
Before your appointment, make a list of:
- Any symptoms your child is experiencing, including any that may seem unrelated to an upper respiratory infection, and when they started
- Key personal information, such as if your child was born prematurely or has a heart or lung problem
- Questions to ask your doctor
Questions to ask your doctor may include the following:
- What is likely causing my child's symptoms? Are there other possible causes?
- Does my child need any tests?
- How long do symptoms usually last?
- Is my child's infection contagious?
- What is the best course of action?
- What are the alternatives to the primary approach that you're suggesting?
- Does my child need medication? If so, is there a generic alternative to the medicine you're prescribing?
- What can I do to make my child feel better?
- Are there any brochures or other printed material that I can have? What websites do you recommend?
Don't hesitate to ask more questions during your appointment.
What to expect from your doctor
Your doctor may ask questions, such as:
- When did your child first begin experiencing symptoms?
- Have your child's symptoms been off and on or continuous?
- How severe are your child's symptoms?
- What, if anything, seems to improve your child's symptoms?
- What, if anything, appears to worsen your child's symptoms?
Your doctor will ask additional questions based on your responses and your child's symptoms and needs. Preparing and anticipating questions will help you make the most of your time with the doctor.
Content Last Updated: January 15, 2020
Content provided by Mayo Clinic ©1998-2026 Mayo Foundation for Medical Education and Research (MFMER). All rights reserved. Terms of Use