Herniated disk
Overview
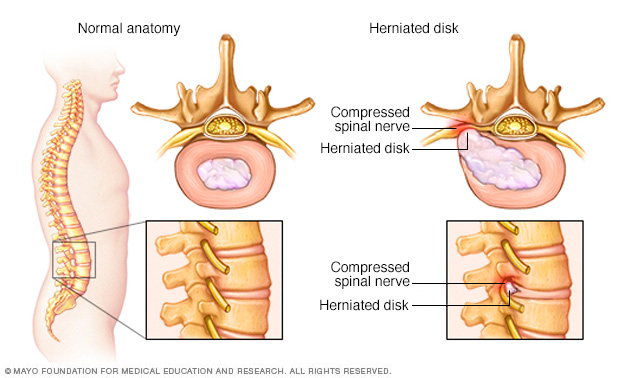
The rubbery disks that lie between the vertebrae in your spine consist of a soft center (nucleus) surrounded by a tougher exterior (annulus). A herniated disk occurs when a portion of the nucleus pushes through a crack in the annulus. Symptoms may occur if the herniation compresses a nerve.
A herniated disk refers to a problem with one of the rubbery cushions (disks) that sit between the individual bones (vertebrae) that stack to make your spine.
A spinal disk has a soft, jellylike center (nucleus) encased in a tougher, rubbery exterior (annulus). Sometimes called a slipped disk or a ruptured disk, a herniated disk occurs when some of the nucleus pushes out through a tear in the annulus.
A herniated disk, which can occur in any part of the spine, can irritate a nearby nerve. Depending on where the herniated disk is, it can result in pain, numbness or weakness in an arm or leg.
Many people have no symptoms from a herniated disk. Surgery is usually not necessary to relieve the problem.
Symptoms
Most herniated disks occur in the lower back, although they can also occur in the neck. Signs and symptoms depend on where the disk is situated and whether the disk is pressing on a nerve. They usually affect one side of the body.
- Arm or leg pain. If your herniated disk is in your lower back, you'll typically feel the most pain in your buttocks, thigh and calf. You might have pain in part of the foot, as well. If your herniated disk is in your neck, you'll typically feel the most pain in your shoulder and arm. This pain might shoot into your arm or leg when you cough, sneeze or move into certain positions. Pain is often described as sharp or burning.
- Numbness or tingling. People who have a herniated disk often have radiating numbness or tingling in the body part served by the affected nerves.
- Weakness. Muscles served by the affected nerves tend to weaken. This can cause you to stumble, or affect your ability to lift or hold items.
You can have a herniated disk without symptoms. You might not know you have it unless it shows up on a spinal image.
When to see a doctor
Seek medical attention if your neck or back pain travels down your arm or leg, or if you also have numbness, tingling or weakness.
Causes
Disk herniation is most often the result of a gradual, aging-related wear and tear called disk degeneration. As you age, your disks become less flexible and more prone to tearing or rupturing with even a minor strain or twist.
Most people can't pinpoint the cause of their herniated disk. Sometimes, using your back muscles instead of your leg and thigh muscles to lift heavy objects can lead to a herniated disk, as can twisting and turning while lifting. Rarely, a traumatic event such as a fall or a blow to the back is the cause.
Risk factors
Factors that can increase your risk of a herniated disk include:
- Weight. Excess body weight causes extra stress on the disks in your lower back.
- Occupation. People with physically demanding jobs have a greater risk of back problems. Repetitive lifting, pulling, pushing, bending sideways and twisting also can increase your risk of a herniated disk.
- Genetics. Some people inherit a predisposition to developing a herniated disk.
- Smoking. It's thought that smoking lessens the oxygen supply to the disk, causing it to break down more quickly.
Complications
Just above your waist, your spinal cord ends. What continues through the spinal canal is a group of long nerve roots that resemble a horse's tail (cauda equina).
Rarely, disk herniation can compress the entire spinal canal, including all the nerves of the cauda equina. Rarely, emergency surgery might be required to avoid permanent weakness or paralysis.
Seek emergency medical attention if you have:
- Worsening symptoms. Pain, numbness or weakness can increase to the point that they hamper your daily activities.
- Bladder or bowel dysfunction. Cauda equina syndrome can cause incontinence or difficulty urinating even with a full bladder.
- Saddle anesthesia. This progressive loss of sensation affects the areas that would touch a saddle — the inner thighs, back of legs and the area around the rectum.
Prevention
To help prevent a herniated disk, do the following:
- Exercise. Strengthening the trunk muscles stabilizes and supports the spine.
- Maintain good posture. This reduces pressure on your spine and disks. Keep your back straight and aligned, particularly when sitting for long periods. Lift heavy objects properly, making your legs — not your back — do most of the work.
- Maintain a healthy weight. Excess weight puts more pressure on the spine and disks, making them more susceptible to herniation.
- Quit smoking. Avoid the use of any tobacco products.
Diagnosis
During the physical exam, your doctor will check your back for tenderness. You might be asked to lie flat and move your legs into various positions to help determine the cause of your pain.
Your doctor may also perform a neurological exam to check your:
- Reflexes
- Muscle strength
- Walking ability
- Ability to feel light touches, pinpricks or vibration
In most cases of herniated disk, a physical exam and a medical history are all that's needed for a diagnosis. If your doctor suspects another condition or needs to see which nerves are affected, he or she may order one or more of the following tests.
Imaging tests
- X-rays. Plain X-rays don't detect herniated disks, but they can rule out other causes of back pain, such as an infection, tumor, spinal alignment issues or a broken bone.
- CT scan. A CT scanner takes a series of X-rays from different directions and then combines them to create cross-sectional images of your spinal column and the structures around it.
- MRI. Radio waves and a strong magnetic field are used to create images of your body's internal structures. This test can be used to confirm the location of the herniated disk and to see which nerves are affected.
- Myelogram. A dye is injected into the spinal fluid before X-rays are taken. This test can show pressure on your spinal cord or nerves due to multiple herniated disks or other conditions.
Nerve tests
Electromyograms and nerve conduction studies measure how well electrical impulses are moving along nerve tissue. This can help pinpoint the location of nerve damage.
- Nerve conduction study. This test measures electrical nerve impulses and functioning in your muscles and nerves through electrodes placed on your skin. The study measures the electrical impulses in your nerve signals when a small current passes through the nerve.
- Electromyography (EMG). During an EMG, your doctor inserts a needle electrode through your skin into various muscles. The test evaluates the electrical activity of your muscles when they contract and when they're at rest.
Treatment
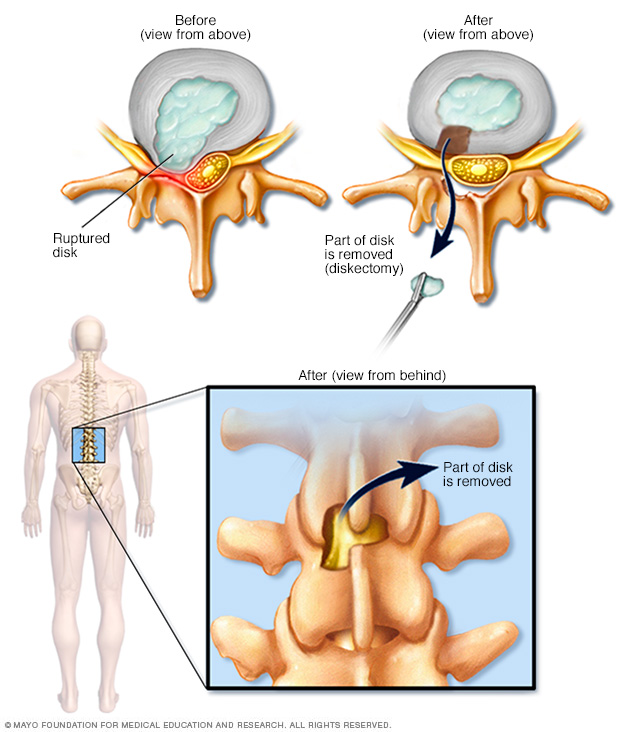
Diskectomy is the surgical removal of the damaged portion of a herniated disk in your spine. A herniated disk occurs when some of the softer material inside the disk pushes out through a crack in the tougher exterior. This can irritate or compress nearby nerves and cause pain, numbness or weakness.
Conservative treatment — mainly modifying activities to avoid movement that causes pain and taking pain medication — relieves symptoms in most people within a few days or weeks.
Medications
- Over-the-counter pain medications. If your pain is mild to moderate, your doctor might recommend over-the-counter pain medication, such as acetaminophen (Tylenol, others) ibuprofen (Advil, Motrin IB, others) or naproxen sodium (Aleve).
- Cortisone injections. If your pain doesn't improve with oral medications, your doctor might recommend a corticosteroid that can be injected into the area around the spinal nerves. Spinal imaging can help guide the needle.
- Muscle relaxers. You might be prescribed these if you have muscle spasms. Sedation and dizziness are common side effects.
- Opioids. Because of the side effects of opioids and the potential for addiction, many doctors hesitate to prescribe them for disk herniation. If other medication doesn't relieve your pain, your doctor might consider short-term use of opioids, such as codeine or an oxycodone-acetaminophen combination (Percocet, Roxicet). Sedation, nausea, confusion and constipation are possible side effects from these drugs.
Therapy
Your doctor might suggest physical therapy to help with your pain. Physical therapists can show you positions and exercises designed to minimize the pain of a herniated disk.
Surgery
Few people with herniated disks eventually need surgery. Your doctor might suggest surgery if conservative treatments fail to improve your symptoms after six weeks, especially if you continue to have:
- Poorly controlled pain
- Numbness or weakness
- Difficulty standing or walking
- Loss of bladder or bowel control
In nearly all cases, surgeons can remove just the protruding portion of the disk. Rarely, the entire disk must be removed. In these cases, the vertebrae may need to be fused with a bone graft.
To allow the process of bone fusion, which takes months, metal hardware is placed in the spine to provide spinal stability. Rarely, your surgeon might suggest the implantation of an artificial disk.
Lifestyle and home remedies
Besides taking the pain medications your doctor recommends, try:
- Applying heat or cold. Initially, cold packs can be used to relieve pain and inflammation. After a few days, you might switch to gentle heat to give relief and comfort.
- Avoiding too much bed rest. Staying in bed can lead to stiff joints and weak muscles — which can complicate your recovery. Instead, rest in a position of comfort for 30 minutes, and then go for a short walk or do some work. Try to avoid activities that worsen your pain.
- Resuming activity slowly. Let your pain guide you in resuming your activities. Make sure your movements are slow and controlled, especially bending forward and lifting.
Alternative medicine
Some alternative and complementary medicine treatments might help ease chronic back pain. Examples include:
- Chiropractic. Spinal manipulation has been found to be moderately effective for low back pain that has lasted for at least a month. Rarely, chiropractic treatment of the neck can cause certain types of strokes.
- Acupuncture. Although results are usually modest, acupuncture appears to ease chronic back and neck pain.
- Massage. This hands-on therapy can provide short-term relief to people dealing with chronic low back pain.
Preparing for an appointment
You're likely to start by seeing your family doctor. You might be referred to a doctor specializing in physical medicine and rehabilitation, orthopedic surgery, neurology, or neurosurgery.
What you can do
Before your appointment, be prepared to answer the following questions:
- When did your symptoms start?
- Were you lifting, pushing or pulling anything at the time you first felt symptoms? Were you twisting your back?
- Has the pain kept you from participating in activities?
- What, if anything, seems to improve your symptoms?
- What, if anything, appears to worsen your symptoms?
- What medications or supplements do you take?
What to expect from your doctor
Your doctor might ask other questions, including:
- Does your pain travel into your arms or legs?
- Do you feel weakness or numbness in your arms or legs?
- Have you noticed changes in your bowel or bladder habits?
- Does coughing or sneezing worsen your leg pain?
- Is the pain interfering with sleep or work?
- Does your work involve heavy lifting?
- Do you smoke or otherwise use tobacco products?
- How has your weight changed recently?
Content Last Updated: September 26, 2019
Content provided by Mayo Clinic ©1998-2026 Mayo Foundation for Medical Education and Research (MFMER). All rights reserved. Terms of Use