Diabetic nephropathy (kidney disease)
Overview
Diabetic nephropathy is a serious complication of type 1 diabetes and type 2 diabetes. It's also called diabetic kidney disease. In the United States, about 1 in 3 people living with diabetes have diabetic nephropathy.
Diabetic nephropathy affects the kidneys' ability to do their usual work of removing waste products and extra fluid from your body. The best way to prevent or delay diabetic nephropathy is by maintaining a healthy lifestyle and adequately managing your diabetes and high blood pressure.
Over many years, the condition slowly damages your kidneys' delicate filtering system. Early treatment may prevent or slow the disease's progress and reduce the chance of complications.
Kidney disease may progress to kidney failure, also called end-stage kidney disease. Kidney failure is a life-threatening condition. At this stage, treatment options are dialysis or a kidney transplant.
Symptoms
In the early stages of diabetic nephropathy, you would most likely not notice any signs or symptoms. In later stages, signs and symptoms may include:
- Worsening blood pressure control
- Protein in the urine
- Swelling of feet, ankles, hands or eyes
- Increased need to urinate
- Reduced need for insulin or diabetes medicine
- Confusion or difficulty concentrating
- Shortness of breath
- Loss of appetite
- Nausea and vomiting
- Persistent itching
- Fatigue
When to see a doctor
Make an appointment with your doctor if you have any signs or symptoms of kidney disease. If you are living with diabetes, visit your doctor yearly — or as recommended — for tests that measure kidney function.
Causes
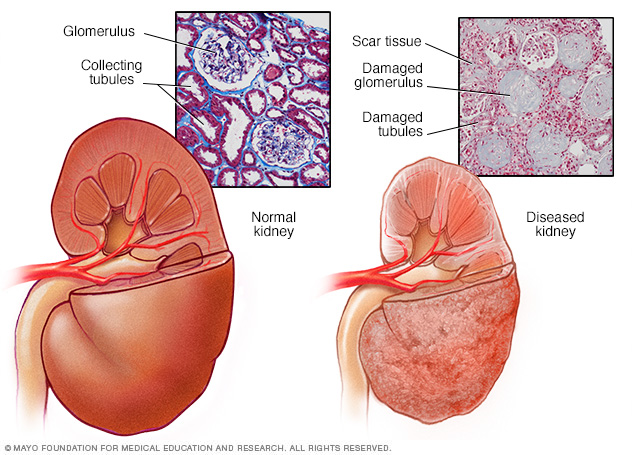
A typical kidney has about 1 million filtering units. Each unit, called a glomerulus, connects to a tubule, which collects urine. Conditions such as high blood pressure and diabetes take a toll on kidney function by damaging these filtering units and collecting tubules and causing scarring.
Diabetic nephropathy results when diabetes damages blood vessels and other cells in your kidneys.
How the kidneys work
Your kidneys contain millions of tiny blood vessel clusters (glomeruli) that filter waste from your blood. Severe damage to these blood vessels can lead to diabetic nephropathy, decreased kidney function and kidney failure.
Diabetic nephropathy causes
Diabetic nephropathy is a common complication of type 1 and type 2 diabetes.
Over time, poorly controlled diabetes can cause damage to blood vessel clusters in your kidneys that filter waste from your blood. This can lead to kidney damage and cause high blood pressure.
High blood pressure can cause further kidney damage by increasing the pressure in the delicate filtering system of the kidneys.
Risk factors
If you're living with diabetes, factors that can increase your risk of diabetic nephropathy include:
- Uncontrolled high blood sugar (hyperglycemia)
- Uncontrolled high blood pressure (hypertension)
- Being a smoker
- High blood cholesterol
- Obesity
- A family history of diabetes and kidney disease
Complications
Complications of diabetic nephropathy may develop gradually over months or years. They may include:
- Fluid retention, which could lead to swelling in your arms and legs, high blood pressure, or fluid in your lungs (pulmonary edema)
- A rise in potassium levels in your blood (hyperkalemia)
- Heart and blood vessel disease (cardiovascular disease), which could lead to stroke
- Damage to the blood vessels of the light-sensitive tissue at the back of the eye (diabetic retinopathy)
- Reduced number of red blood cells to transport oxygen (anemia)
- Foot sores, erectile dysfunction, diarrhea and other problems related to damaged nerves and blood vessels
- Bone and mineral disorders due to the inability of the kidneys to maintain the right balance of calcium and phosphorus in the blood
- Pregnancy complications that carry risks for the mother and the developing fetus
- Irreversible damage to your kidneys (end-stage kidney disease), eventually needing either dialysis or a kidney transplant for survival
Prevention
To reduce your risk of developing diabetic nephropathy:
- Keep regular appointments for diabetes management. Keep annual appointments — or more-frequent appointments if recommended by your health care team — to monitor how well you are managing your diabetes and to screen for diabetic nephropathy and other complications.
- Treat your diabetes. With effective treatment of diabetes, you may prevent or delay diabetic nephropathy.
- Manage high blood pressure or other medical conditions. If you have high blood pressure or other conditions that increase your risk of kidney disease, work with your doctor to control them.
- Follow instructions on over-the-counter medications. Follow instructions on the packages of nonprescription pain relievers such as aspirin and nonsteroidal anti-inflammatory drugs, such as naproxen (Aleve) and ibuprofen (Advil, Motrin IB, others). For people with diabetic nephropathy, taking these types of pain relievers can lead to kidney damage.
- Maintain a healthy weight. If you're at a healthy weight, work to maintain it by being physically active most days of the week. If you need to lose weight, talk with your doctor about weight-loss strategies, such as increasing daily physical activity and consuming fewer calories.
- Don't smoke. Cigarette smoking can damage your kidneys and make existing kidney damage worse. If you're a smoker, talk to your doctor about strategies for quitting smoking. Support groups, counseling and some medications can all help you to stop.
Diagnosis
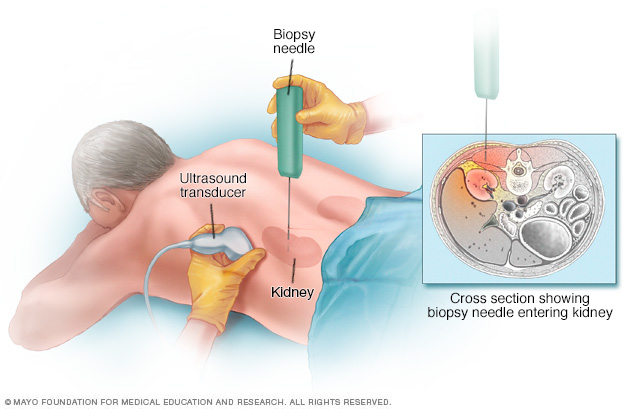
During a kidney biopsy, your doctor uses a needle to remove a small sample of kidney tissue for lab testing. The biopsy needle is inserted through your skin and is often directed using the guidance of an imaging device, such as an ultrasound transducer.
Diabetic nephropathy is usually diagnosed during routine testing that's a part of your diabetes management. If you're living with type 1 diabetes, screening for diabetic nephropathy is recommended beginning five years after your diagnosis. If you are diagnosed with type 2 diabetes, screening will begin at the time of diagnosis.
Routine screening tests may include:
- Urinary albumin test. This test can detect the blood protein albumin in your urine. Typically, the kidneys don't filter albumin out of the blood. Too much of the protein in your urine can indicate poor kidney function.
- Albumin/creatinine ratio. Creatinine is a chemical waste product that healthy kidneys filter out of the blood. The albumin/creatinine ratio — a measure of how much albumin is in a urine sample relative to how much creatinine there is — provides another indication of kidney function.
- Glomerular filtration rate (GFR). The measure of creatinine in a blood sample may be used to estimate how quickly the kidneys filter blood (glomerular filtration rate). A low filtration rate indicates poor kidney function.
Other diagnostic tests may include the following:
- Imaging tests. Your doctor may use X-rays and ultrasound to assess your kidneys' structure and size. You may also undergo CT scanning and magnetic resonance imaging (MRI) to determine how well blood is circulating within your kidneys. Other imaging tests may be used in some cases.
- Kidney biopsy. Your doctor may recommend a kidney biopsy to take a sample of kidney tissue. You'll be given a numbing medication (local anesthetic). Then your doctor will use a thin needle to remove small pieces of kidney tissue for examination under a microscope.
Treatment
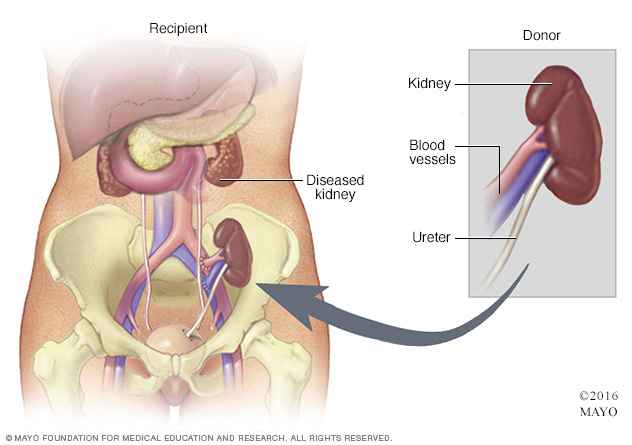
During kidney transplant surgery, the donor kidney is placed in your lower abdomen. Blood vessels of the new kidney are attached to blood vessels in the lower part of your abdomen, just above one of your legs. The new kidney's ureter is connected to your bladder. Unless they are causing complications, your own kidneys are left in place.
The first step in treating diabetic nephropathy is to treat and control your diabetes and high blood pressure (hypertension). This includes diet, lifestyle changes, exercise and prescription medications. With good management of your blood sugar and hypertension, you may prevent or delay kidney dysfunction and other complications.
Medications
In the early stages of diabetic nephropathy, your treatment plan may include medications to manage the following:
- Blood pressure control. Medications called angiotensin-converting enzyme (ACE) inhibitors and angiotensin 2 receptor blockers (ARBs) are used to treat high blood pressure.
- Blood sugar control. Medications can help control high blood sugar in people with diabetic nephropathy. Metformin (Fortamet, Glumetza, others) improves insulin sensitivity and lowers glucose production in the liver. Glucagon-like peptide 1 (GLP-1) receptor agonists help lower blood sugar levels by slowing digestion and stimulating insulin secretion in response to rising glucose levels. SGLT2 inhibitors limit the return of glucose to the bloodstream, leading to increased glucose excretion in the urine.
- High cholesterol. Cholesterol-lowering drugs called statins are used to treat high cholesterol and reduce protein in the urine.
- Kidney scarring. Finerenone (Kerendia) disrupts molecular activity believed to cause inflammation and tissue scarring in diabetic nephropathy. Research has shown that the drug may reduce the risk of kidney function decline, kidney failure, cardiovascular death, nonfatal heart attacks and hospitalization for heart failure in adults with chronic kidney disease associated with type 2 diabetes.
Your doctor will likely recommend follow-up testing at regular intervals to see whether your kidney disease remains stable or progresses.
Treatment for advanced diabetic nephropathy
If your disease progresses to kidney failure (end-stage kidney disease), your doctor will likely discuss options for care focused on either replacing the function of your kidneys or making you more comfortable. Options include:
- Kidney dialysis. This treatment removes waste products and extra fluid from your blood. The two main types of dialysis are hemodialysis and peritoneal dialysis. In the first, more common method, you may need to visit a dialysis center and be connected to an artificial kidney machine about three times a week, or you may have dialysis done at home by a trained caregiver. Each session takes 3 to 5 hours. The second method may be done at home as well.
- Transplant. In some situations, the best option is a kidney transplant or a kidney-pancreas transplant. If you and your doctor decide on transplantation, you'll be evaluated to determine whether you're eligible for this surgery.
- Symptom management. If you choose not to have dialysis or a kidney transplant, your life expectancy generally would be only a few months. You may receive treatment to help keep you comfortable.
Potential future treatments
In the future, people with diabetic nephropathy may benefit from treatments being developed using regenerative medicine. These techniques may help reverse or slow kidney damage caused by the disease. For example, some researchers think that if a person's diabetes can be cured by a future treatment such as pancreas islet cell transplant or stem cell therapy, kidney function may improve. These therapies, as well as new medications, are still under investigation.
Lifestyle and home remedies
Diet, exercise and self-management are essential for controlling blood sugar levels and high blood pressure. Your diabetes care team will help you with the following goals:
- Monitor your blood sugar level. Your health care provider will advise you on how often to check your blood sugar level to make sure you remain within your target range. You may, for example, need to check it once a day and before or after exercise. If you take insulin, you may need to check it multiple times a day.
- Be active most days of the week. Aim for at least 30 minutes or more of moderate to vigorous aerobic exercise — such as brisk walking, swimming, biking or running — on most days for a total of at least 150 minutes a week.
- Eat a healthy diet. Eat a high-fiber diet with lots of fruits, nonstarchy vegetables, whole grains and legumes. Limit saturated fats, processed meats, sweets and sodium.
- Quit smoking. If you're a smoker, talk with your doctor about strategies for quitting smoking.
- Maintain a healthy weight. If you need to lose weight, talk with your doctor about weight-loss strategies. For some people, weight-loss surgery is an option.
- Take a daily aspirin. Talk with your doctor about whether you should take a daily low-dose aspirin to lower the risk of cardiovascular disease.
- Be vigilant. Alert doctors unfamiliar with your medical history that you have diabetic nephropathy. They can take steps to protect your kidneys from further damage by avoiding medical tests that use contrast dye, such as angiograms and computerized tomography scans.
Coping and support
If you have diabetic nephropathy, these steps may help you cope:
- Connect with other people who have diabetes and kidney disease. Ask your doctor about support groups in your area. Or contact organizations such as the American Association of Kidney Patients, the National Kidney Foundation or the American Kidney Fund for groups in your area.
- Maintain your usual routine, when possible. Try to maintain your usual routine, doing the activities you enjoy and continuing to work, if your condition allows. This may help you cope with feelings of sadness or loss that you may experience after your diagnosis.
- Talk with someone you trust. Living with diabetic nephropathy can be stressful, and it may help to talk about your feelings. You may have a friend or family member who is a good listener. Or you may find it helpful to talk with a faith leader or someone else you trust. Consider asking your doctor for a referral to a social worker or counselor.
Preparing for an appointment
Diabetic nephropathy is usually identified during regular appointments for diabetes care. After a diagnosis of diabetic nephropathy, your overall treatment plan will address ongoing management of diabetes and tests to monitor changes in kidney function.
If you've been recently diagnosed with diabetic nephropathy, you may want to discuss the following questions with your doctor:
- How well are my kidneys functioning now?
- What treatments do you recommend?
- How do these treatments change or fit into my overall diabetes treatment plan?
- How will we know if these treatments are working?
Questions for ongoing appointments
Before any appointment with a member of your diabetes treatment team, ask whether you need to follow any restrictions, such as fasting before taking a test. Questions to regularly review with your doctor or other members of the team include:
- How often should I monitor my blood sugar, and what is my target range?
- What changes in my diet would help me better manage my blood sugar, cholesterol or blood pressure?
- What is the right dosage for prescribed medications?
- When should I take the medications? Do I take them with food?
- How is management of diabetes affecting treatment for other conditions? How can I better coordinate treatments or care?
- When do I need to make a follow-up appointment?
- Under what conditions should I call you or seek emergency care?
- Are there brochures or online sources you recommend?
- Are there resources available if I'm having trouble paying for diabetes supplies?
What to expect from your doctor
Your health care provider is likely to ask you a number of questions at regularly scheduled appointments, including:
- Do you understand your treatment plan and feel confident you can follow it?
- How are you coping with diabetes?
- Have you experienced any low blood sugar?
- Do you know what to do if your blood sugar is too low or too high?
- What's a typical day's diet like?
- Are you exercising? If so, what type of exercise? How often?
- Do you sit for long periods of time?
- What challenges are you experiencing in managing your diabetes?
Content Last Updated: October 19, 2021
Content provided by Mayo Clinic ©1998-2026 Mayo Foundation for Medical Education and Research (MFMER). All rights reserved. Terms of Use