Wolff-Parkinson-White (WPW) syndrome
Overview
In Wolff-Parkinson-White (WPW) syndrome, an extra electrical pathway between your heart's upper chambers and lower chambers causes a rapid heartbeat.
In Wolff-Parkinson-White (WPW) syndrome, an extra electrical pathway between your heart's upper and lower chambers causes a rapid heartbeat. The condition, which is present at birth, is fairly rare.
The episodes of fast heartbeats usually aren't life-threatening, but serious heart problems can occur. Treatment can stop or prevent episodes of fast heartbeats. A catheter-based procedure (ablation) can permanently correct the heart rhythm problems.
Most people with an extra electrical pathway have no fast heartbeat. This condition, called Wolff-Parkinson-White pattern, is discovered by chance during a heart exam.
Symptoms
Anyone, even babies, can have the symptoms of WPW syndrome, which result from changes in heart rhythm.
Common symptoms of WPW syndrome include:
- A rapid, fluttering or pounding heartbeat (palpitations)
- Dizziness or lightheadedness
- Shortness of breath
- Fatigue
- Anxiety
- Chest pain
- Difficulty breathing
- Fainting
An episode of a fast heartbeat can begin suddenly and last a few seconds or several hours. Episodes can occur during exercise or while at rest. Caffeine or other stimulants and alcohol trigger symptoms for some people.
Symptoms in infants
Signs and symptoms in infants with WPW syndrome can include:
- Grayish or blueish (ashen) skin color
- Restlessness or irritability
- Rapid breathing
- Poor eating
When to see a doctor
A number of conditions can cause irregular heartbeat (arrhythmia). It's important to get a prompt diagnosis and care. See your doctor if you or your child has symptoms of WPW syndrome.
Call 911 or your local emergency number if you have any of the following symptoms for more than a few minutes:
- Rapid or irregular heartbeat
- Difficulty breathing
- Chest pain
Causes
In a typical heart rhythm, a tiny cluster of cells at the sinus node sends out an electrical signal. The signal then travels through the atria to the atrioventricular (AV) node and into the ventricles, causing them to contract and pump blood.
The extra electrical pathway that causes a rapid heartbeat is present at birth. An abnormal gene is the cause in a small percentage of people with WPW. The syndrome also is associated with some forms of congenital heart disease, such as Ebstein anomaly.
Otherwise, little is known about why the extra pathway develops.
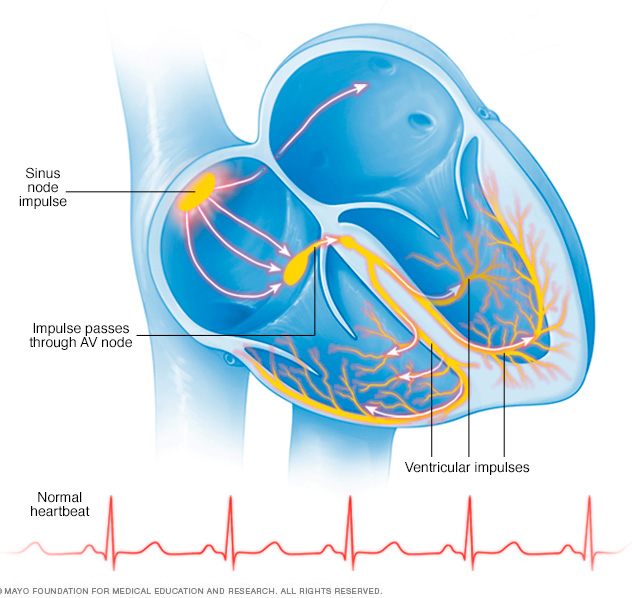
Normal heart electrical system
Your heart is made up of four chambers — two upper chambers (atria) and two lower chambers (ventricles). The rhythm of your heart is normally controlled by a mass of tissue in the right atrium (sinus node). The sinus node produces electrical impulses, or signals, that cause each heartbeat.
These electrical signals travel across the atria, causing muscle contractions that pump blood into the ventricles. The signals then arrive at a cluster of cells called the atrioventricular (AV) node — usually the only pathway for signals to travel from the atria to the ventricles. The AV node slows the electrical signal before sending it to the ventricles.
This slight delay allows the ventricles to fill with blood. When the electrical signals reach the ventricles, muscle contractions pump blood to the lungs and the rest of the body.
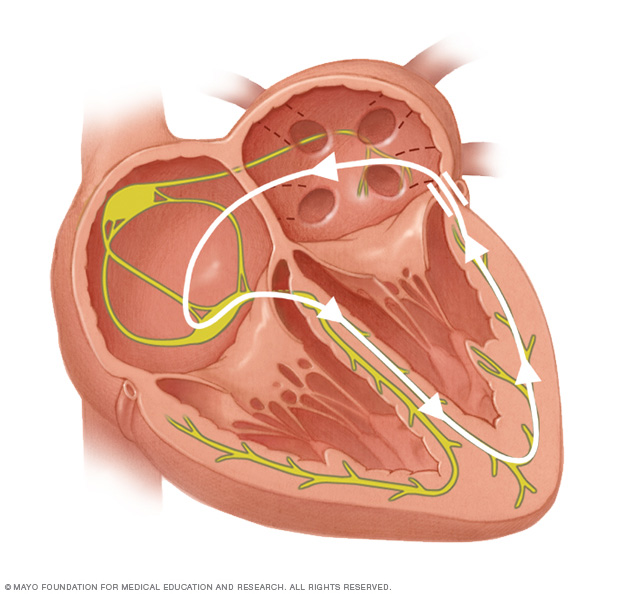
Abnormal electrical system in WPW
In WPW syndrome, an extra electrical pathway connects the atria and ventricles, allowing electrical impulses to bypass the AV node. This detour activates the ventricles too early.
The extra pathway can also transmit electrical impulses from the ventricles back to the atria, disrupting the coordinated movement of the electrical signals through the heart, leading to changes in the heart rhythm.
The most common arrhythmia associated with WPW syndrome is called paroxysmal supraventricular tachycardia. Some people with WPW syndrome have a type of irregular heartbeat known as atrial fibrillation.
Complications
For many people, WPW syndrome doesn't cause serious problems. But complications can occur. It's not always possible to know your risk of serious heart-related events. If WPW syndrome is untreated — particularly if you have other heart conditions — you might have:
- Fainting spells
- Fast heartbeats
- Rarely, sudden cardiac arrest
Diagnosis
Your doctor will likely recommend tests to diagnose WPW syndrome, such as:
- Electrocardiogram (ECG). Small sensors attached to your chest and arms record electrical signals as they travel through your heart. Your doctor can look for patterns among these signals that indicate an extra electrical pathway in your heart.
- Holter monitor. A Holter monitor is a portable ECG device at home that you wear when you're away from the doctor's office. The device records your heart's activity while you perform your everyday activities for a day or two. An event recorder monitors heart activity when your heart beats too fast. Some personal devices, such as smart watches, offer ECG monitoring. Ask your doctor if this is an option for you.
- Electrophysiological testing. Thin, flexible tubes (catheters) tipped with electrodes are threaded through your blood vessels to various spots in your heart. The electrodes map the spread of electrical impulses during each heartbeat and identify an extra electrical pathway.
Treatment
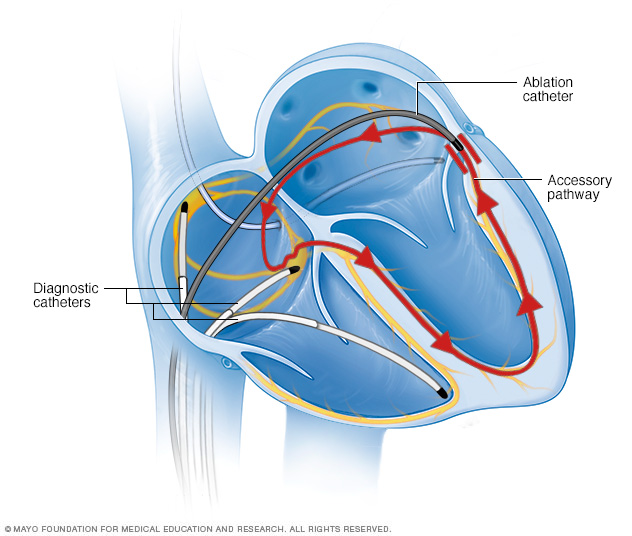
In catheter ablation, catheters are threaded through the blood vessels to the inner heart, and electrodes at the catheter tips map the spread of electrical impulses through the heart. Electrodes at the catheter tips transmit energy to destroy a small spot of heart tissue and create an electrical block along the pathway that's causing your arrhythmia.
Treatment depends on several factors, including the severity and frequency of your symptoms and the type of arrhythmia you have.
If you have the WPW pathway but don't have symptoms, you probably won't need treatment. If you do, the goal of treatment is to slow a fast heart rate when it occurs and to prevent future episodes.
Treatment options include:
- Vagal maneuvers. These simple physical movements — which include coughing, bearing down as if you are having a bowel movement and putting an ice pack on your face — affect a nerve that helps regulate your heartbeat (vagus nerve). Your doctor might suggest you do vagal maneuvers to help slow a rapid heartbeat when it occurs.
- Medications. If vagal maneuvers don't stop the fast heartbeat, you might need an injection of an anti-arrhythmic medication. Your doctor also might recommend a medication that can slow the heart rate.
- Cardioversion. Paddles or patches on your chest can electrically shock your heart and help restore a normal rhythm. Cardioversion is typically used when maneuvers and medications aren't effective.
- Radiofrequency catheter ablation. Thin, flexible tubes (catheters) are threaded through blood vessels to your heart. Electrodes at the catheter tips are heated to destroy (ablate) the extra electrical pathway causing your condition. Radiofrequency ablation permanently corrects the heart-rhythm problems in most people with WPW syndrome.
Preparing for an appointment
Here's some information to help you get ready for your appointment.
What you can do
When you make the doctor's appointment, be sure to ask if you need to do anything in advance, such as restrict your or your child's diet.
Write down the following information and take it with you to the appointment:
- Your or your child's symptoms, including any that may seem unrelated to your heart, and when they began
- All medications, vitamins or other supplements you or your child takes, including doses
- Key medical information, including other diagnosed conditions
- Key personal information, including any recent life changes or stressors
- Write down questions to ask your doctor
If you're seeing a new doctor, request that a copy of medical records be sent to the new office.
Questions to ask your doctor
- What's the most likely cause of my symptoms?
- What tests do I need?
- What treatments can help?
- What risks does this heart condition create?
- How often will I need follow-up appointments?
- Do I need to restrict activities?
- How will other conditions that I have or medications I take affect my heart problem?
What to expect from your doctor
Your doctor is likely to ask you questions, such as:
- How severe are the symptoms?
- How often have you or your child had a fast heartbeat?
- How long have the episodes lasted?
- Does anything (such as exercise, stress or caffeine) seem to trigger the episodes or make symptoms worse?
- Do you have a family history of heart disease?
Content Last Updated: February 12, 2020
Content provided by Mayo Clinic ©1998-2026 Mayo Foundation for Medical Education and Research (MFMER). All rights reserved. Terms of Use