Pectus excavatum
Overview
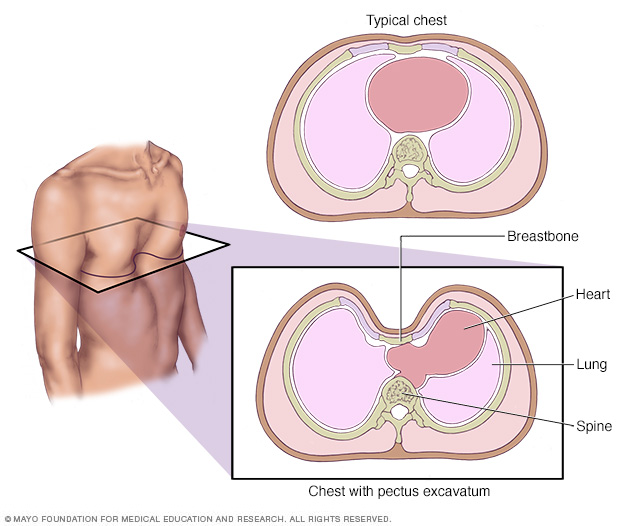
Pectus excavatum is a condition in which a person's breastbone is sunken into his or her chest. Severe cases of pectus excavatum can eventually interfere with the function of the heart and lungs.
Pectus excavatum is a condition in which a person's breastbone is sunken into his or her chest. In severe cases, pectus excavatum can look as if the center of the chest has been scooped out, leaving a deep dent.
While the sunken breastbone is often noticeable shortly after birth, the severity of pectus excavatum typically worsens during the adolescent growth spurt.
Also called funnel chest, pectus excavatum is more common in boys than in girls. Severe cases of pectus excavatum can eventually interfere with the function of the heart and lungs. But even mild cases of pectus excavatum can make children feel self-conscious about their appearance. Surgery can correct the deformity.
Symptoms
For many people with pectus excavatum, the only sign or symptom is a slight indentation in their chests. In some people, the depth of the indentation worsens in early adolescence and can continue to worsen into adulthood.
In severe cases of pectus excavatum, the breastbone may compress the lungs and heart. Signs and symptoms may include:
- Decreased exercise tolerance
- Rapid heartbeat or heart palpitations
- Recurrent respiratory infections
- Wheezing or coughing
- Chest pain
- Heart murmur
- Fatigue
- Dizziness
Causes
While the exact cause of pectus excavatum is unknown, it may be an inherited condition because it sometimes runs in families.
Risk factors
Pectus excavatum is more common in boys than in girls. It also occurs more often in people who also have:
- Marfan syndrome
- Ehlers-Danlos syndrome
- Osteogenesis imperfecta
- Noonan syndrome
- Turner syndrome
Complications
Severe cases of pectus excavatum can compress the heart and lungs or push the heart over to one side. Even mild cases of pectus excavatum can result in self-image problems.
Heart and lung problems
If the depth of the breastbone indentation is severe, it may reduce the amount of room the lungs have to expand. This compression can also squeeze the heart, pushing it into the left side of the chest and reducing its ability to pump efficiently. This can cause symptoms such as exercise intolerance, shortness of breath, rapid heart rate and chest pain.
Self-image problems
Many people who have pectus excavatum will also tend to have a hunched-forward posture, with flared ribs and shoulder blades. Many are so self-conscious about their appearance that they avoid activities, such as swimming, that make the indentation in their chests more difficult to camouflage behind clothing.
Diagnosis
Pectus excavatum can usually be diagnosed simply by examining the chest. Your doctor may suggest several different types of tests to check for associated problems with the heart and lungs. These tests may include:
- Chest X-ray. This test can visualize the dip in the breastbone and often shows the heart being displaced into the left side of the chest. X-rays are painless and take only a few minutes to complete.
- Computerized tomography (CT). A CT scan may be used to help determine the severity of the pectus excavatum and whether the heart or lungs are being compressed. CT scans take many X-rays from a variety of angles to produce cross-sectional images of the body's internal structure. You may be asked to undergo a special CT that looks at the effects of the compression on the heart while breathing in and out.
- Electrocardiogram. An electrocardiogram can show whether the heart's rhythm is normal or irregular, and if the electrical signals that control the heartbeat are timed properly. This test is painless and involves the placement of more than a dozen electrical leads, which are attached to the body with a sticky adhesive. It is common for a patient with pectus to have an abnormal EKG.
- Echocardiogram. An echocardiogram is a sonogram of the heart. It can show real-time images of how well the heart and its valves are working. The images are produced by transmitting sound waves via a wand pressed against the chest. An echocardiogram also gives your doctor a look at how the chest wall may be affecting heart function and the flow of blood through the heart.
- Lung function tests. These types of tests measure the amount of air your lungs can hold and how quickly you can empty your lungs.
- Exercise test. This test monitors how well your heart and lungs function while you exercise, usually on a bike or treadmill.
Treatment
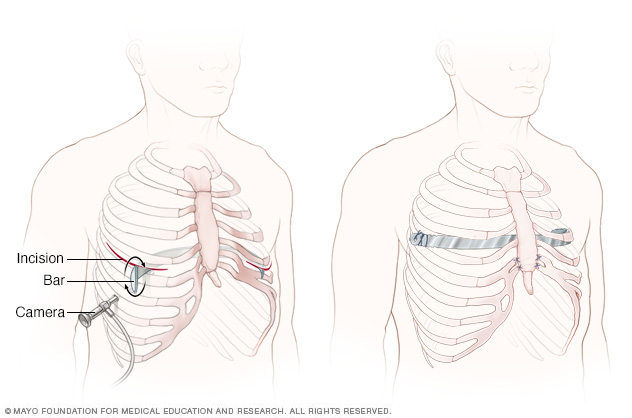
The Nuss procedure inserts a curved metal bar through small incisions on each side of the chest. The bar is then flipped to press upwards on the breastbone. In some cases, more than one bar is used.
Pectus excavatum can be surgically repaired, but surgery is usually reserved for people who have moderate to severe signs and symptoms. People who have mild signs and symptoms may be helped by physical therapy. Certain exercises can improve posture and increase the degree to which the chest can expand.
If the depression of your breastbone isn't causing any symptoms but you're unhappy with how it looks, you could talk to a surgeon about having a silicone insert — similar to a breast implant — placed under your skin to fill in that space.
Repair surgery
The two most common surgical procedures to repair pectus excavatum are known by the names of the surgeons who first developed them:
- Nuss procedure. This minimally invasive procedure uses small incisions placed on each side of the chest. Long-handled tools and a narrow fiber-optic camera are inserted through the incisions. A curved metal bar is threaded under the depressed breastbone, to raise it into a more normal position. In some cases, more than one bar is used. The bars are removed after two or three years.
- Ravitch technique. This older procedures involves a much larger incision down the center of the chest. The surgeon removes the deformed cartilage attaching the ribs to the lower breastbone and then fixes the breastbone into a more normal position with surgical hardware, such as a metal strut or mesh supports. These supports are removed in six to 12 months.
Most people who undergo surgery to correct pectus excavatum are happy with the change in how their chests look, no matter which procedure is used. Although most surgeries for pectus excavatum are performed around the growth spurt at puberty, many adults also have benefitted from pectus excavatum repair.
Temporarily freezing the nerves to block pain (cryoablation) can help with recovery and decrease postoperative pain for four to six weeks.
Potential future treatments
Doctors are currently studying therapies that use suction or magnets to help raise the depressed breastbone. These devices are best used in younger patients. As people age, the chest becomes more rigid, which limits chest wall movement.
Coping and support
Most adolescents just want to fit in and look like their peers. This can be exceptionally difficult for youngsters who have pectus excavatum. In some cases, counseling may be needed to help master coping skills. Online support groups and forums also are available, where you can talk with people who are facing the same types of problems.
Preparing for an appointment
If you or your child has pectus excavatum, you might first discuss the condition with your family doctor. He or she may refer you to a doctor who specializes in pediatric or thoracic surgery.
What you can do
You may want to write a list that includes:
- Detailed descriptions of your signs and symptoms
- Information about past medical problems
- Information about medical problems common in your family
- All the medications and dietary supplements you or your child takes
- Questions you want to ask the doctor, including what treatments are available
What to expect from your doctor
Your doctor may ask some of the following questions:
- When did these signs and symptoms begin?
- Have they worsened recently?
- Has anyone else in your family had a similar problem?
Content Last Updated: April 29, 2020
Content provided by Mayo Clinic ©1998-2026 Mayo Foundation for Medical Education and Research (MFMER). All rights reserved. Terms of Use