Gastroparesis
Overview
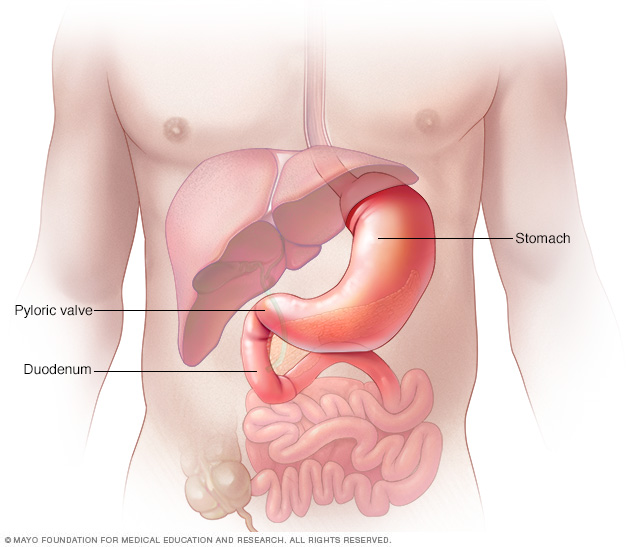
Your stomach is a muscular sac about the size of a small melon that expands when you eat or drink to hold as much as a gallon (about 4 liters) of food or liquid. Once your stomach pulverizes the food, strong muscular contractions (peristaltic waves) push the food toward the pyloric valve, which leads to the upper portion of your small intestine (duodenum).
Gastroparesis is a condition that affects the normal spontaneous movement of the muscles (motility) in your stomach. Ordinarily, strong muscular contractions propel food through your digestive tract. But if you have gastroparesis, your stomach's motility is slowed down or doesn't work at all, preventing your stomach from emptying properly.
The cause of gastroparesis is usually unknown. Sometimes it's a complication of diabetes, and some people develop gastroparesis after surgery. Certain medications, such as opioid pain relievers, some antidepressants, and high blood pressure and allergy medications, can lead to slow gastric emptying and cause similar symptoms. For people who already have gastroparesis, these medications may make their condition worse.
Gastroparesis can interfere with normal digestion, cause nausea, vomiting and abdominal pain. It can also cause problems with blood sugar levels and nutrition. Although there's no cure for gastroparesis, changes to your diet, along with medication, can offer some relief.
Symptoms
Signs and symptoms of gastroparesis include:
- Vomiting
- Nausea
- Abdominal bloating
- Abdominal pain
- A feeling of fullness after eating just a few bites
- Vomiting undigested food eaten a few hours earlier
- Acid reflux
- Changes in blood sugar levels
- Lack of appetite
- Weight loss and malnutrition
Many people with gastroparesis don't have any noticeable signs and symptoms.
When to see a doctor
Make an appointment with your doctor if you have any signs or symptoms that worry you.
Causes
It's not always clear what leads to gastroparesis, but in some cases it can be caused by damage to a nerve that controls the stomach muscles (vagus nerve).
The vagus nerve helps manage the complex processes in your digestive tract, including signaling the muscles in your stomach to contract and push food into the small intestine. A damaged vagus nerve can't send signals normally to your stomach muscles. This may cause food to remain in your stomach longer, rather than move into your small intestine to be digested.
The vagus nerve and its branches can be damaged by diseases, such as diabetes, or by surgery to the stomach or small intestine.
Risk factors
Factors that can increase your risk of gastroparesis:
- Diabetes
- Abdominal or esophageal surgery
- Infection, usually from a virus
- Certain medications that slow the rate of stomach emptying, such as narcotic pain medications
- Scleroderma — a connective tissue disease
- Nervous system diseases, such as Parkinson's disease or multiple sclerosis
- Underactive thyroid (hypothyroidism)
Women are more likely to develop gastroparesis than are men.
Complications
Gastroparesis can cause several complications, such as:
- Severe dehydration. Ongoing vomiting can cause dehydration.
- Malnutrition. Poor appetite can mean you don't take in enough calories, or you may be unable to absorb enough nutrients due to vomiting.
- Undigested food that hardens and remains in your stomach. Undigested food in your stomach can harden into a solid mass called a bezoar. Bezoars can cause nausea and vomiting and may be life-threatening if they prevent food from passing into your small intestine.
- Unpredictable blood sugar changes. Although gastroparesis doesn't cause diabetes, frequent changes in the rate and amount of food passing into the small bowel can cause erratic changes in blood sugar levels. These variations in blood sugar make diabetes worse. In turn, poor control of blood sugar levels makes gastroparesis worse.
- Decreased quality of life. Symptoms can make it difficult to work and keep up with other responsibilities.
Diagnosis
Doctors use several tests to help diagnose gastroparesis and rule out conditions that may cause similar symptoms. Tests may include:
Gastric emptying tests
To see how fast your stomach empties its contents, one or more of these tests may be recommended:
-
Scintigraphy. This is the most important test used in making a diagnosis of gastroparesis. It involves eating a light meal, such as eggs and toast, that contains a small amount of radioactive material. A scanner that detects the movement of the radioactive material is placed over your abdomen to monitor the rate at which food leaves your stomach.
You'll need to stop taking any medications that could slow gastric emptying. Ask your doctor if any of your medications might slow your digestion.
- Breath tests. For breath tests, you consume a solid or liquid food that contains a substance that your body absorbs. Eventually, the substance can be detected in your breath. Samples of your breath are collected over a few hours and the amount of the substance in your breath is measured. The test can show how fast your stomach empties after consuming food by measuring the amount of the substance in your breath.
Upper gastrointestinal (GI) endoscopy
This procedure is used to visually examine your upper digestive system — your esophagus, stomach and beginning of the small intestine (duodenum). It uses a tiny camera on the end of a long, flexible tube. This test can also be used to diagnose other conditions, such as peptic ulcer disease or pyloric stenosis, which can have symptoms similar to those of gastroparesis.
Ultrasound
This test uses high-frequency sound waves to produce images of structures within your body. Ultrasound can help diagnose whether problems with your gallbladder or your kidneys could be causing your symptoms.
Treatment
Treating gastroparesis begins with identifying and treating the underlying condition. If diabetes is causing your gastroparesis, your doctor can work with you to help you control it.
Changes to your diet
Maintaining adequate nutrition is the most important goal in the treatment of gastroparesis. Many people can manage gastroparesis with dietary changes. Your doctor may refer you to a dietitian who can work with you to find foods that are easier for you to digest. This can help you to get enough calories and nutrients from the food you eat.
A dietitian might suggest that you try to:
- Eat smaller meals more frequently
- Chew food thoroughly
- Eat well-cooked fruits and vegetables rather than raw fruits and vegetables
- Avoid fibrous fruits and vegetables, such as oranges and broccoli, which may cause bezoars
- Choose mostly low-fat foods, but if you can tolerate fat, add small servings of fatty foods to your diet
- Try soups and pureed foods if liquids are easier for you to swallow
- Drink about 34 to 51 ounces (1 to 1.5 liters) of water a day
- Exercise gently after you eat, such as going for a walk
- Avoid carbonated drinks, alcohol and smoking
- Try to avoid lying down for two hours after a meal
- Take a multivitamin daily
Ask your dietitian for a comprehensive list of foods recommended for people with gastropareses. Here's a brief list:
Starches
- White bread and rolls and whole-wheat bread without nuts or seeds
- Plain or egg bagels
- English muffins
- Flour or corn tortillas
- Pancakes
- Puffed wheat and rice cereals
- Cream of Wheat or rice
- White crackers
- Potatoes, white or sweet (no skin)
- Baked french fries
- Rice
- Pasta
Protein
- Lean beef, veal and pork (not fried)
- Chicken or turkey (no skin and not fried)
- Crab, lobster, shrimp, clams, scallops, oysters
- Tuna (packed in water)
- Cottage cheese
- Eggs
- Tofu
- Strained meat baby food
Fruits and vegetables
- Pureed vegetables and fruits, such as baby food
- Tomato sauce, paste, puree, juice
- Carrots (cooked)
- Beets (cooked)
- Mushrooms (cooked)
- Vegetable juice
- Vegetable broth
- Fruit juices and drinks
- Applesauce
- Bananas
- Peaches and pears (canned)
Dairy
- Milk, if tolerated
- Yogurt (without fruit pieces)
- Custard and pudding
- Frozen yogurt
Medications
Medications to treat gastroparesis may include:
-
Medications to stimulate the stomach muscles. These medications include metoclopramide (Reglan) and erythromycin. Metoclopramide has a risk of serious side effects. Erythromycin may lose its effectiveness over time, and can cause side effects, such as diarrhea.
A newer medication, domperidone, with fewer side effects, is also available with restricted access.
- Medications to control nausea and vomiting. Drugs that help ease nausea and vomiting include diphenhydramine (Benadryl, others) and ondansetron (Zofran). Prochlorperazine (Compro) is used if nausea and vomiting persist.
Surgical treatment
Some people with gastroparesis may be unable to tolerate any food or liquids. In these situations, doctors may recommend a feeding tube (jejunostomy tube) be placed in the small intestine. Or doctors may recommend a gastric venting tube to help relieve pressure from gastric contents.
Feeding tubes can be passed through your nose or mouth or directly into your small intestine through your skin. The tube is usually temporary and is only used when gastroparesis is severe or when blood sugar levels can't be controlled by any other method. Some people may require an IV (parenteral) feeding tube that goes directly into a vein in the chest.
Treatments under investigation
Researchers are continuing to investigate new medications to treat gastroparesis.
One example is a new drug in development called Relamorelin. The results of a phase II trial found the drug could speed up gastric emptying and reduce vomiting. The drug is not yet approved in the United States by the Food and Drug Administration (FDA), but a larger clinical trial is currently underway.
A number of new therapies are being tried with the help of endoscopy — a procedure done with a slender tube (endoscope) that's threaded down the esophagus.
One procedure, known as endoscopic pyloromyotomy (gastric peroral endoscopic myotomy, or G-POEM), involves making an incision in the valve or muscular ring between the stomach and small intestine called the pylorus. A channel is then opened from the stomach to the small intestine. This is a relatively recent procedure that shows promise, though additional research is needed.
Another type of endoscopic procedure involves placing a small tube (stent) where the stomach connects to the small intestine (duodenum) to keep this connection open.
Gastric electrical stimulation and pacing
In gastric electrical stimulation, a surgically implanted device provides electrical stimulation to the stomach muscles to move food more efficiently. Study results have been mixed. However, the device seems to be most helpful for people with diabetic gastroparesis.
The FDA allows the device to be used under a compassionate use exemption for those who can't control their gastroparesis symptoms with diet changes or medications. However, larger studies are needed.
Lifestyle and home remedies
If you're a smoker, stop. Your gastroparesis symptoms are less likely to improve over time if you keep smoking.
Alternative medicine
Some complementary and alternative therapies have been used to treat gastroparesis, including acupuncture. Acupuncture involves the insertion of extremely thin needles through your skin at strategic points on your body. During electroacupuncture, a small electrical current is passed through the needles. Studies have shown these treatments may ease gastroparesis symptoms more than a sham treatment.
Preparing for an appointment
You're likely to first see your primary care doctor if you have signs and symptoms of gastroparesis. If your doctor suspects you may have gastroparesis, you may be referred to a doctor who specializes in digestive diseases (gastroenterologist). You may also be referred to a dietitian who can help you choose foods that are easier to process.
What you can do
Because appointments can be brief, it's a good idea to be well-prepared. To prepare, try to:
- Be aware of any pre-appointment restrictions. At the time you make the appointment, be sure to ask if there's anything you need to do in advance, such as restrict your diet. Your doctor's office might recommend that you stop using certain pain medications, such as narcotics, prior to coming for an appointment.
- Write down any symptoms you're experiencing, including any that may seem unrelated to the reason for which you scheduled the appointment.
- Write down key personal information, including any major stresses or recent life changes.
- Make a list of all medications, vitamins or supplements that you're taking.
- Consider taking a family member or friend along. Sometimes it can be difficult to remember all the information provided during an appointment. Someone who accompanies you may remember something that you missed or forgot.
- Write down questions to ask your doctor.
Questions to ask
Your time with your doctor is limited, so preparing a list of questions will help you make the most of your time together. List your questions from most important to least important in case time runs out. For gastroparesis, some basic questions to ask your doctor include:
- What's the most likely cause of my symptoms?
- Could any of my medications be causing my signs and symptoms?
- What kinds of tests do I need?
- Is this condition temporary or long lasting?
- Do I need treatment for my gastroparesis?
- What are my treatment options, and what are the potential side effects?
- Are there certain foods I can eat that are easier to digest?
- I have other health conditions. How can I best manage these conditions together?
- Should I see a dietitian?
- Should I see a specialist? What will that cost, and will my insurance cover it?
- Are there brochures or other printed material that I can take with me? What websites do you recommend?
- Do I need a follow-up visit?
- I have diabetes. How might gastroparesis affect my diabetes management?
In addition to the questions that you've prepared, don't hesitate to ask other questions during your appointment.
What to expect from your doctor
Your doctor is likely to ask you a number of questions. Being ready to answer them may allow more time later to cover other points you want to address. Your doctor may ask:
- When did you first begin experiencing symptoms?
- Have your symptoms been continuous or occasional?
- How severe are your symptoms?
- Does anything seems to improve your symptoms?
- What, if anything, appears to worsen your symptoms?
- Did your symptoms start suddenly, such as after an episode of food poisoning?
- What surgeries have you had?
Content Last Updated: October 10, 2020
Content provided by Mayo Clinic ©1998-2026 Mayo Foundation for Medical Education and Research (MFMER). All rights reserved. Terms of Use