Head lice
Overview
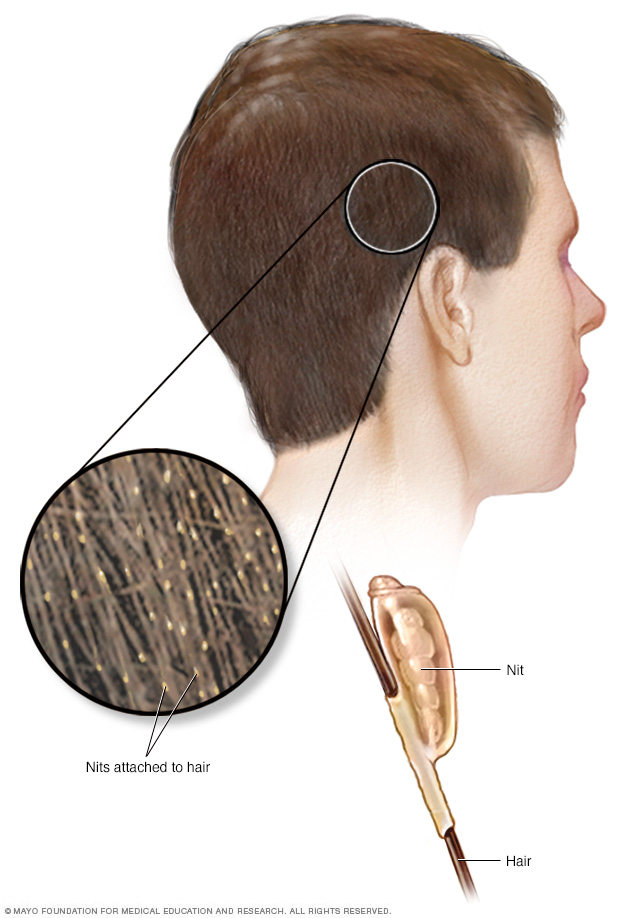
Head lice feed on blood from the scalp. The female louse lays eggs (nits) that stick to hair shafts.
Head lice are tiny insects that feed on blood from the human scalp. An infestation of head lice most often affects children and usually results from the direct transfer of lice from the hair of one person to the hair of another.
A head-lice infestation isn't a sign of poor personal hygiene or an unclean living environment. Head lice don't carry bacterial or viral infectious diseases.
Over-the-counter and prescription medications are available to treat head lice. Follow treatment instructions carefully to rid your scalp and hair of lice and their eggs.
A number of home or natural remedies are also used to treat head-lice infestations, but there is little to no clinical evidence of their effectiveness.
Symptoms
Common signs and symptoms of a lice infestation can include:
- Itching. The most common symptom of a lice infestation is itching on the scalp, neck and ears. This is an allergic reaction to louse bites. When a person has a lice infestation for the first time, itching may not occur for four to six weeks after infestation.
- Lice on scalp. Lice may be visible but are difficult to spot because they're small, avoid light and move quickly.
- Lice eggs (nits) on hair shafts. Nits stick to hair shafts. Incubating nits may be difficult to see because they're very tiny. They're easiest to spot around the ears and the hairline of the neck. Empty nits may be easier to spot because they're lighter in color and further from the scalp. However, the presence of nits doesn't necessarily indicate an active infestation.
- Sores on the scalp, neck and shoulders. Scratching can lead to small, red bumps that may sometimes get infected with bacteria.
When to see a doctor
See your doctor before you begin treatment if you suspect that you or your child has a head-lice infestation. Studies show that many children have been treated for head lice with over-the-counter medications or home remedies when they don't have an active head-lice infestation.
Things often mistaken for nits include:
- Dandruff
- Residue from hair products
- Bead of dead hair tissue on a hair shaft (hair cast)
- Scabs, dirt or other debris
- Other small insects found in the hair
Causes
A head louse is a tan or grayish insect about the size of a strawberry seed. It feeds on human blood from a person's scalp. The female louse produces a sticky substance that firmly attaches each egg to the base of a hair shaft no more than 3/16 inch (5 millimeters) from the scalp.
The louse life cycle
A louse goes through three stages:
- Eggs that hatch after six to nine days.
- Nymphs, immature forms of the louse that become mature adults after nine to 12 days.
- Adult lice, which can live for three to four weeks. The female louse lays six to 10 eggs a day.
Transmission
Head lice crawl, but they can't jump or fly. Transmission of a head louse from one person to another is often by direct head-to-head contact, often within a family or among children who have close contact at school or play.
Indirect transmission is uncommon, but lice may spread from one person to another by items such as:
- Hats and scarves
- Brushes and combs
- Hair accessories
- Headphones
- Pillows, towels and upholstery
Indirect transfer could also occur among items of clothing stored together. For example, hats or scarves hung on the same hook or stored in the same school locker could serve as vehicles for transmitting lice.
Household pets, such as dogs and cats, don't play a role in spreading head lice.
Risk factors
Because head lice are spread primarily by direct head-to-head contact, the risk of transmission is greatest among younger people who play or go to school together. In the United States, cases of head lice most often occur in children in preschool through elementary school.
Complications
If your child scratches an itchy scalp from a head-lice infestation, it is possible for the skin to break and develop an infection.
Prevention
It's difficult to prevent the spread of head lice among children in child care facilities and schools because there is so much close contact.
The chance of indirect transmission from personal items is slight. However, to help prevent a head-lice infestation, you may instruct your child to:
- Hang garments on a separate hook from other children's garments
- Avoid sharing combs, brushes, hats and scarves
- Not lie on beds, couches or pillows that have been in contact with a person infested by head lice
A worry about head-lice transmission is not considered a good reason to avoid sharing protective headgear for sports and bicycling when sharing is necessary.
Diagnosis
According to the American Academy of Pediatrics guidelines, the gold standard for diagnosing an active head-lice infestation is the identification of a live nymph or adult louse.
These guidelines recommend an examination of wet hair lubricated with such products as a standard hair conditioner. Your doctor will carefully comb your child's hair with a fine-toothed comb (nit comb) from the scalp to the end of the hair. If no live louse is found, he or she will likely repeat the entire exam at a second appointment.
Identifying nits
Your doctor will also look for nits in your child's hair. To find nits, he or she may use a specialized light called a Wood's light, which causes nits to appear bluish. But the identification of nits does not necessarily confirm the diagnosis of an active lice infestation.
A live nit needs to be near the scalp to survive. Nits found more than about 1/4 inch (6 millimeters) from the scalp are likely dead or empty. Suspect nits can be examined under a microscope to determine if they're living — evidence of a likely active lice infestation.
If no live nits are found, they're probably left from a previous infestation and do not need to be treated.
Treatment
Your doctor will likely recommend an over-the-counter (OTC) medication that kills lice and some of the nits. These medications may not kill recently laid eggs. Therefore, an appropriately timed second treatment is usually necessary to kill nymphs after they hatch but before they become adult lice.
Some studies suggest that retreating seven to nine days after the first treatment is the ideal time for a second treatment, but other retreatment schedules exist. Ask your doctor for written instructions for a recommended treatment schedule.
Over-the-counter (OTC) products
OTC medications are based on pyrethrin, a chemical compound extracted from the chrysanthemum flower that is toxic to lice. Wash your child's hair with shampoo with no conditioner before using one of these treatments. Rinsing the hair with white vinegar before washing may help dissolve the glue that holds the nits to the hair shafts. Follow directions on the package for how long to leave the medication in the hair, and rinse your child's hair over a sink with warm water.
OTC medications include the following:
- Permethrin (Nix). Permethrin is a synthetic version of pyrethrin. Permethrin does not kill nits, and treatment needs to be repeated nine to 10 days after first application. Side effects may include redness and itching of the scalp.
- Pyrethrin with additives (Rid). In this OTC medication, pyrethrin is combined with another chemical that enhances its effectiveness. This product only kills lice, not nits, and needs to be reapplied nine to 10 days after first treatment. Side effects may include itching and redness of the scalp. Pyrethrin shouldn't be used if your child is allergic to chrysanthemum or ragweed.
Prescription medications
In some geographic regions, lice have developed resistance to OTC medications. Also, OTC treatment may fail because of incorrect use, such as not repeating the treatment at an appropriate time.
If the correct use of an OTC treatment has failed, your doctor may recommend a prescription treatment. These include:
- Ivermectin (Sklice). Ivermectin is toxic to lice. It is approved for use with people age 6 months or older. It can be applied once to dry hair and then rinsed with water after 10 minutes. Ivermectin is also available as a tablet to be taken by mouth to children weighing more than 33 lbs. if other topical treatments do not effectively eliminate a lice infestation.
- Spinosad (Natroba). Spinosad is approved for use with people age 6 months or older. It can be applied to dry hair and rinsed with warm water after 10 minutes. It kills lice and nits and usually doesn't need repeated treatment.
- Malathion. Malathion is approved for use with people age 6 or older. The lotion is applied, left to dry naturally and rinsed out after eight to 12 hours. The drug has a high alcohol content, so it can't be used with a hair dryer or near an open flame. Malathion can be reapplied seven to nine days after the first treatment if necessary.
Lifestyle and home remedies
If you prefer not to use a medication for treating a head-lice infestation, you may consider an alternative home treatment. There is little to no clinical evidence of the effectiveness of such treatments.
Wet-combing
Combing wet hair with a fine-toothed nit comb may remove lice and some nits. Studies show that wet-combing results vary.
The hair should be wet, and you should add something to lubricate the hair, such as a hair conditioner or olive oil. Comb the entire head from the scalp to the end of the hair at least twice during a session. The process should be repeated every three to four days for several weeks — at least two weeks after no more lice are found.
Essential oils
Small clinical studies have suggested that some natural plant oils may kill lice by suffocation, but effectiveness is uncertain. These products include:
- Tea tree oil
- Anise oil
- Ylang-ylang oil
These products are not required to meet safety, efficacy and manufacturing standards used for drugs approved by the Food and Drug Administration (FDA), and can sometimes cause allergic reactions.
Smothering agents
A number of household products are used to treat head-lice infestations. These products are thought to deprive the lice of air when generous amounts are applied to the hair, covered with a shower cap and left on overnight. Products used for this purpose include:
- Mayonnaise
- Olive oil
- Margarine or butter
- Petroleum jelly
However, the effectiveness of these treatments is unclear.
Dehydration
Another option is a machine that uses one application of hot air in an attempt to kill head lice and their eggs through dehydration. The machine requires special training and is currently available only at professional lice treatment centers.
The machine uses air that is cooler than most hair dryers and at a much higher flow rate to kill the lice by drying them out. A regular hair dryer should not be used to accomplish this result as it's too hot and could burn the scalp.
Dangerous products to avoid
Flammable products, such as kerosene or gasoline, should never be used to kill lice or to remove nits.
Household cleaning
Lice usually don't live past one day without feeding from a human scalp, and eggs do not survive if they aren't incubated at the temperature near the scalp. Therefore, the chance of lice surviving on household items is small.
As a precaution, you may clean items that the affected person has used in the previous two days. Cleaning recommendations include the following:
- Wash items in hot water. Wash bedding, stuffed animals and clothing in hot, soapy water — at least 130 F (54.4 C) — and dry at high heat.
- Clean hair care items. Clean combs, brushes and hair accessories by soaking them in hot, soapy water for five to 10 minutes.
- Seal items in plastic bags. Seal items that can’t be washed in plastic bags for two weeks.
- Vacuum. Give the floor and upholstered furniture a good vacuuming.
Preparing for an appointment
See your family doctor or pediatrician if you suspect your child has head lice. Your doctor will examine your child's scalp and look for a live nymph or adult louse to determine if he or she has an active head-lice infestation. Your doctor can carefully inspect your child's hair and, if necessary, examine suspect items under a microscope before confirming a diagnosis of head-lice infestation.
Content Last Updated: July 10, 2020
Content provided by Mayo Clinic ©1998-2026 Mayo Foundation for Medical Education and Research (MFMER). All rights reserved. Terms of Use