Aortic valve stenosis
Overview
Aortic valve stenosis — or aortic stenosis — occurs when the heart's aortic valve narrows. The valve doesn't open fully, which reduces or blocks blood flow from your heart into the main artery to your body (aorta) and to the rest of your body.
Your treatment depends on the severity of your condition. You may need surgery to repair or replace the valve. Without treatment, severe aortic valve stenosis can lead to death.
Symptoms
Aortic valve stenosis ranges from mild to severe. Signs and symptoms generally occur when narrowing of the valve is severe. Some people with aortic valve stenosis may not have symptoms for many years.
Signs and symptoms of aortic valve stenosis may include:
- Abnormal heart sound (heart murmur) heard through a stethoscope
- Chest pain (angina) or tightness with activity
- Feeling faint or dizzy or fainting with activity
- Shortness of breath, especially when you have been active
- Fatigue, especially during times of increased activity
- Rapid, fluttering heartbeat (palpitations)
- Not eating enough (mainly in children with aortic valve stenosis)
- Not gaining enough weight (mainly in children with aortic valve stenosis)
Aortic valve stenosis may lead to heart failure. Heart failure signs and symptoms include fatigue, shortness of breath, and swollen ankles and feet.
When to see a doctor
If you have a heart murmur, your doctor may recommend that you visit a doctor trained in diseases of the heart (cardiologist). If you develop any symptoms that may suggest aortic valve stenosis, see your doctor.
Causes
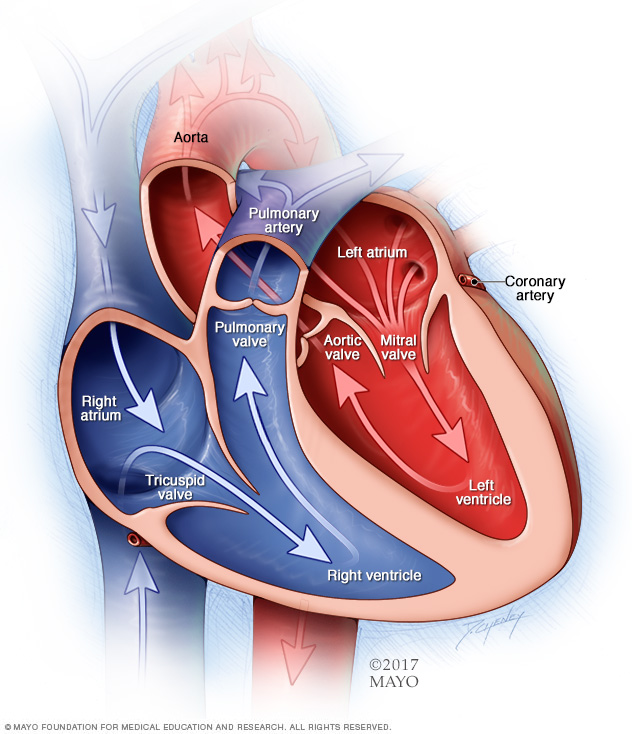
A typical heart has two upper and two lower chambers. The upper chambers — the right and left atria — receive incoming blood. The lower chambers — the right and left ventricles — pump blood out of the heart. The heart valves, which keep blood flowing in the right direction, are gates at the chamber openings (for the tricuspid and mitral valves) and exits (for the pulmonary and aortic valves).
Your heart has four valves that keep blood flowing in the correct direction. These valves include the mitral valve, tricuspid valve, pulmonary valve and aortic valve. Each valve has flaps (cusps or leaflets) that open and close once during each heartbeat. Sometimes, the valves don't open or close properly. If a valve doesn't fully open or close, blood flow is reduced or blocked.
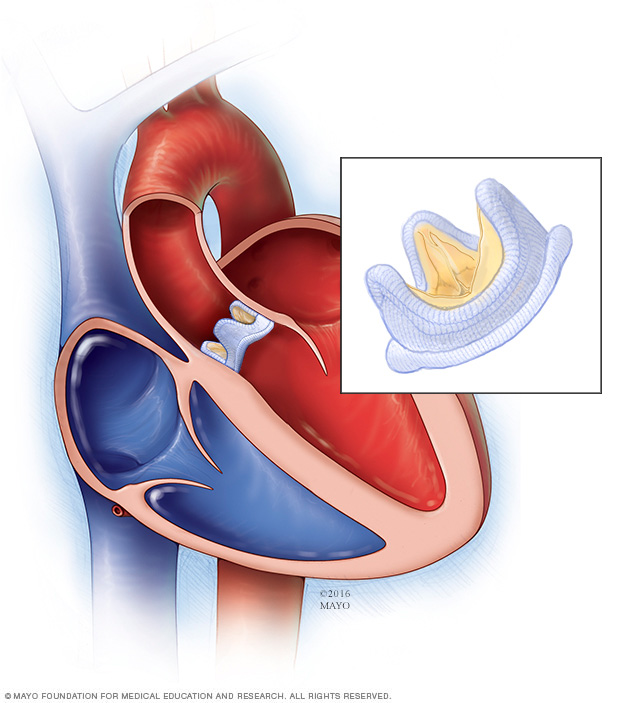
In aortic valve stenosis, the aortic valve between the lower left heart chamber (left ventricle) and the aorta does not open completely. The area through which blood moves out of the heart to the aorta is narrowed (stenosis).
When the aortic valve opening is narrowed, your heart must work harder to pump enough blood into the aorta and to the rest of your body. The extra work of the heart can cause the left ventricle to thicken and enlarge. Eventually the strain can cause a weakened heart muscle and can ultimately lead to heart failure and other serious problems.
Aortic valve stenosis causes include:
-
Congenital heart defect. Some children are born with an aortic valve that has only two cusps (bicuspid aortic valve) instead of three (tricuspid aortic valve). Rarely, an aortic valve may have one (unicuspid) or four (quadricuspid) cusps.
Having a congenital heart defect such as a bicuspid aortic valve requires regular checkups by a doctor. The valve defect may not cause any problems until adulthood. If the valve begins to narrow or leak, it may need to be repaired or replaced.
-
Calcium buildup on the valve. Calcium is a mineral found in your blood. As blood repeatedly flows over the aortic valve, calcium deposits can build up on the heart valves (aortic valve calcification).
The calcium deposits may never cause any problems. Aortic valve stenosis that's related to increasing age and calcium deposit buildup usually doesn't cause symptoms until ages 70 or 80. However, in some people — particularly those with a congenital aortic valve defect — calcium deposits result in stiffening of the valve cusps at a younger age.
Heart valve calcium deposits aren't linked to taking calcium tablets or drinking calcium-fortified products.
-
Rheumatic fever. This complication of strep throat infection may result in scar tissue forming on the aortic valve. Scar tissue can narrow the aortic valve opening or create a rough surface on which calcium deposits can collect.
Rheumatic fever may damage more than one heart valve, and in more than one way. While rheumatic fever is rare in the United States, some older adults had rheumatic fever as children.
Risk factors
Risk factors of aortic valve stenosis include:
- Older age
- Certain heart conditions present at birth (congenital heart disease) such as a bicuspid aortic valve
- History of infections that can affect the heart
- Having cardiovascular risk factors, such as diabetes, high cholesterol and high blood pressure
- Chronic kidney disease
- History of radiation therapy to the chest
Complications
Aortic valve stenosis can cause complications, including:
- Heart failure
- Stroke
- Blood clots
- Bleeding
- Heart rhythm problems (arrhythmias)
- Infections that affect the heart, such as endocarditis
- Death
Prevention
Some possible ways to prevent aortic valve stenosis include:
- Taking steps to prevent rheumatic fever. You can do this by making sure that you see your doctor when you have a sore throat. Untreated strep throat can develop into rheumatic fever. Fortunately, strep throat can usually be easily treated with antibiotics. Rheumatic fever is more common in children and young adults.
- Addressing risk factors for coronary artery disease. These include high blood pressure, obesity and high cholesterol levels. These factors may be linked to aortic valve stenosis, so it's a good idea to keep your weight, blood pressure and cholesterol levels under control if you have aortic valve stenosis.
- Taking care of your teeth and gums. There may be a link between infected gums (gingivitis) and infected heart tissue (endocarditis). Inflammation of heart tissue caused by infection can narrow arteries and aggravate aortic valve stenosis.
Once you know that you have aortic valve stenosis, your doctor may recommend that you limit strenuous activity to avoid overworking your heart.
Diagnosis
To diagnose aortic valve stenosis, your doctor will review your signs and symptoms, discuss your medical history, and do a physical examination. He or she will listen to your heart with a stethoscope to determine if you have a heart murmur that may signal an aortic valve condition.
Tests
Your doctor may order several tests to confirm or rule out aortic valve stenosis. Tests also can help determine a cause and the condition's severity.
Tests for aortic valve stenosis may include:
-
Echocardiogram. This test uses sound waves to create images of your heart in motion. A technician presses a device (transducer) firmly against your skin, aiming an ultrasound beam through your chest to your heart. The transducer records the sound wave echoes from your heart, and a computer converts the echoes into images that your doctor can view on a monitor.
An echocardiogram can show your doctor how blood flows through your heart and heart valves. It can help identify a weakened heart muscle and determine the severity of aortic valve stenosis.
If your doctor needs a closer look at your aortic valve, a transesophageal echocardiogram may be done. In this test, a flexible tube containing the transducer is guided down your throat and into your esophagus.
- Electrocardiogram (ECG or EKG). This painless test detects and records your heart's electrical activity using small sensors (electrodes) attached to your chest and arms and, sometimes, legs. An EKG can detect enlarged chambers of your heart, heart disease and abnormal heart rhythms.
- Chest X-ray. A chest X-ray can help your doctor determine whether your heart is enlarged, which can occur in aortic valve stenosis. It can also show swelling of the aorta and calcium buildup on your aortic valve.
- Exercise tests or stress tests. Exercise tests help your doctor determine whether signs and symptoms of aortic valve disease occur during physical activity. These tests can help determine the severity of your condition. If you are unable to exercise, medications that have similar effects as exercise on your heart may be given to complete the test.
- Cardiac computerized tomography (CT) scan. A cardiac CT scan combines several X-ray images to provide a more detailed cross-sectional view of the heart. Doctors may use cardiac CT to measure the size of your aorta and look at your aortic valve more closely.
- Cardiac MRI. A cardiac MRI uses magnetic fields and radio waves to create detailed images of your heart. This test may be used to determine the severity of your condition and evaluate the size of your aorta.
-
Cardiac catheterization. This test isn't often used to diagnose aortic valve disease, but it may be used if other tests aren't able to diagnose the condition or to determine its severity. It may also be used before aortic valve surgery to make sure the arteries that feed the heart muscle (coronary arteries) are not blocked.
In this procedure, your doctor threads a thin tube (catheter) through a blood vessel in your arm or groin and guides it to an artery in your heart.
Sometimes, dye is injected through the catheter to help your arteries show up more clearly on an X-ray (coronary angiogram). A coronary angiogram gives your doctor a detailed picture of your heart arteries and how your heart functions. During the test, your doctor can also measure the pressure inside your heart chambers.
Treatment
In biological valve replacement, a valve made from cow, pig or human heart tissue replaces the damaged valve.
Treatment for aortic valve stenosis depends on your signs and symptoms and the severity of the condition.
If you have mild symptoms or none at all, you may only need to have your condition monitored with regular doctor's appointments. Your doctor may recommend healthy lifestyle changes and medications to treat symptoms or reduce the risk of complications.
Surgery or other procedures
You may eventually need surgery to repair or replace the diseased aortic valve, even if you don't have symptoms. Aortic valve surgery may be done at the same time as other heart surgery.
Surgery to repair or replace an aortic valve is usually done through a cut (incision) in the chest. Less invasive approaches may be available. Ask your doctor if you're a candidate for these procedures. Aortic valve surgery may be done at the same time as other heart surgery.
Surgery options for aortic valve stenosis include:
- Aortic valve repair. To repair an aortic valve, surgeons separate valve flaps (cusps) that have fused. However, surgeons rarely repair an aortic valve to treat aortic valve stenosis. Generally aortic valve stenosis requires aortic valve replacement.
-
Balloon valvuloplasty. This procedure can treat aortic valve stenosis in infants and children. However, the valve tends to narrow again in adults who've had the procedure, so it's usually only done in adults who are too ill for surgery or who are waiting for a valve replacement, as they typically need additional procedures to treat the narrowed valve over time.
In this procedure, a doctor inserts a long, thin tube (catheter) with a balloon on the tip into an artery in your arm or groin and guides it to the aortic valve. Once in place, the balloon is inflated, which widens the valve opening. The balloon is then deflated, and the catheter and balloon are removed.
-
Aortic valve replacement. Aortic valve replacement is often needed to treat aortic valve stenosis. In aortic valve replacement, your surgeon removes the damaged valve and replaces it with a mechanical valve or a valve made from cow, pig or human heart tissue (biological tissue valve).
Biological tissue valves break down over time and may eventually need to be replaced. People with mechanical valves will need to take blood-thinning medications for life to prevent blood clots. Your doctor will discuss with you the benefits and risks of each type of valve.
-
Transcatheter aortic valve replacement (TAVR). This less invasive procedure may be an option for people who are considered to be at intermediate or high risk of complications from surgical aortic valve replacement.
In TAVR, doctors insert a catheter in your leg or chest and guide it to your heart. A replacement valve is then inserted through the catheter and guided to your heart. A balloon may expand the valve, or some valves can self-expand. When the valve is implanted, doctors remove the catheter from your blood vessel. Doctors may also perform a catheter procedure to insert a replacement valve into a biological tissue valve that is no longer working properly.
Lifestyle and home remedies
You'll have regular follow-up appointments with your doctor to monitor your condition. You'll need to continue taking all your medications as prescribed.
Your doctor may suggest that you incorporate several heart-healthy lifestyle changes into your life, including:
- Eating a heart-healthy diet. Eat a variety of fruits and vegetables, low-fat or fat-free dairy products, poultry, fish, and whole grains. Avoid saturated and trans fat, and excess salt and sugar.
- Maintaining a healthy weight. Aim to keep a healthy weight. If you're overweight or obese, your doctor may recommend that you lose weight.
- Getting regular physical activity. Aim to include about 30 minutes of physical activity, such as brisk walks, into your daily fitness routine.
- Managing stress. Find ways to help manage your stress, such as through relaxation activities, mindfulness, exercise, and spending time with family and friends.
- Avoiding tobacco. If you smoke, quit. Ask your doctor about resources to help you quit smoking. Joining a support group may be helpful.
For women with aortic valve stenosis, it's important to talk with your doctor before you become pregnant. Together, you and your doctor can discuss which medications are safe to take during pregnancy, and whether you may need a procedure to treat your valve condition before getting pregnant.
You'll likely require close monitoring by your doctor during pregnancy. Doctors may recommend that women with severe valve stenosis avoid pregnancy to avoid the risk of complications.
Preparing for an appointment
If you think you have aortic valve stenosis, consider being evaluated and treated at a medical center with a multidisciplinary team of cardiologists and other doctors and medical staff trained and experienced in evaluating and treating heart valve disease.
Here's some information to help you prepare for your appointment.
What you can do
- Be aware of pre-appointment restrictions. When you make the appointment, ask if there's anything you need to do beforehand.
- Write down your symptoms, including any that seem unrelated to heart valve disease.
- Write down key personal information, including a family history of heart disease and any major stresses or recent life changes.
- Make a list of all medications, vitamins and supplements you take.
- Take a family member or friend along, if possible. Someone who accompanies you can help you remember information you receive.
- Be prepared to discuss your diet and exercise habits. If you don't already eat well and exercise, be ready to talk to your doctor about challenges you might face in getting started.
- Write down questions to ask your doctor.
For aortic valve stenosis, some basic questions to ask your doctor include:
- What is likely causing my symptoms or condition?
- What are other possible causes for my symptoms or condition?
- What tests will I need?
- What's the best treatment?
- What are the alternatives to the primary approach you're suggesting?
- I have other health conditions. How can I best manage them together?
- Are there restrictions I need to follow?
- Should I see a specialist?
- If I need surgery, which surgeon do you recommend for heart valve surgery?
- Is there a generic alternative to the medicine you're prescribing?
- Are there brochures or other printed material I can take with me? What websites do you recommend?
Don't hesitate to ask other questions you have.
What to expect from your doctor
Your doctor is likely to ask you a number of questions, including:
- When did your symptoms begin?
- Do you always have symptoms or do they come and go?
- How severe are your symptoms?
- What, if anything, improves your symptoms?
- What, if anything, worsens your symptoms?
Content Last Updated: February 26, 2021
Content provided by Mayo Clinic ©1998-2026 Mayo Foundation for Medical Education and Research (MFMER). All rights reserved. Terms of Use