Presbyopia
Overview
Presbyopia is the gradual loss of your eyes' ability to focus on nearby objects. It's a natural, often annoying part of aging. Presbyopia usually becomes noticeable in your early to mid-40s and continues to worsen until around age 65.
You may become aware of presbyopia when you start holding books and newspapers at arm's length to be able to read them. A basic eye exam can confirm presbyopia. You can correct the condition with eyeglasses or contact lenses. You might also consider surgery.
Symptoms
Presbyopia develops gradually. You may first notice these signs and symptoms after age 40:
- A tendency to hold reading material farther away to make the letters clearer
- Blurred vision at normal reading distance
- Eyestrain or headaches after reading or doing close-up work
You may notice these symptoms are worse if you are tired or are in an area with dim lighting.
When to see a doctor
See an eye doctor if blurry close-up vision is keeping you from reading, doing close-up work or enjoying other normal activities. He or she can determine whether you have presbyopia and advise you of your options.
Seek immediate medical care if you:
- Have a sudden loss of vision in one eye with or without eye pain
- Experience sudden hazy or blurred vision
- See flashes of light, black spots or halos around lights
- Have double vision
Causes
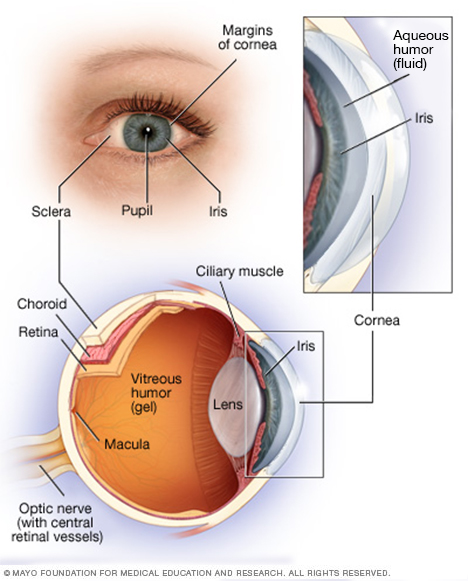
Your eye is a complex and compact structure measuring about 1 inch (2.5 centimeters) in diameter. It receives millions of pieces of information about the outside world, which are quickly processed by your brain.
To form an image, your eye relies on the cornea and the lens to focus the light reflected from objects. The closer the object, the more the lens flexes.
- The cornea is the clear, dome-shaped front surface of your eye.
- The lens is a clear structure about the size and shape of an M&M's candy.
- Both of these structures bend (refract) light entering your eye to focus the image on the retina, located on the inside back wall of your eye.
The lens, unlike the cornea, is somewhat flexible and can change shape with the help of a circular muscle that surrounds it. When you look at something at a distance, the circular muscle relaxes. When you look at something nearby, the muscle constricts, allowing the relatively elastic lens to curve and change its focusing power.
Presbyopia is caused by a hardening of the lens of your eye, which occurs with aging. As your lens becomes less flexible, it can no longer change shape to focus on close-up images. As a result, these images appear out of focus.
Risk factors
Certain factors can make you more likely to develop presbyopia, including:
- Age. Age is the greatest risk factor for presbyopia. Almost everyone experiences some degree of presbyopia after age 40.
- Other medical conditions. Being farsighted or having certain diseases — such as diabetes, multiple sclerosis or cardiovascular diseases — can increase your risk of premature presbyopia, which is presbyopia in people younger than 40.
- Drugs. Certain drugs are associated with premature presbyopic symptoms, including antidepressants, antihistamines and diuretics.
Diagnosis
Presbyopia is diagnosed by a basic eye exam, which includes a refraction assessment and an eye health exam.
A refraction assessment determines if you have nearsightedness or farsightedness, astigmatism, or presbyopia. Your doctor may use various instruments and ask you to look through several lenses to test your distance and close-up vision.
Your eye doctor likely will put drops in your eyes to dilate your pupils for the eye health exam. This may make your eyes more light sensitive for a few hours after the exam. Dilation enables your doctor to more easily view the inside of your eyes.
The American Academy of Ophthalmology recommends that adults have a complete eye exam every:
- Five to 10 years under age 40
- Two to four years between ages 40 and 54
- One to three years between ages 55 and 64
- One to two years beginning at age 65
You may need more-frequent exams if you have risk factors for eye disease or you need glasses or contact lenses.
Treatment
The goal of treatment is to compensate for the inability of your eyes to focus on nearby objects. Treatment options include wearing corrective eyeglasses (spectacle lenses) or contact lenses, undergoing refractive surgery, or getting lens implants for presbyopia.
Eyeglasses
Eyeglasses are a simple, safe way to correct vision problems caused by presbyopia. You may be able to use over-the-counter (nonprescription) reading glasses if you had good, uncorrected vision before developing presbyopia. Ask your eye doctor if nonprescription glasses are OK for you.
Most nonprescription reading glasses range in power from +1.00 diopter (D) to +3.00 D. When selecting reading glasses:
- Try different powers until you find the magnification that allows you to read comfortably, starting with the lower powers
- Test each pair on reading material held at a comfortable distance
You'll need prescription lenses for presbyopia if over-the-counter glasses are inadequate or if you already require prescription corrective lenses for nearsightedness, farsightedness or astigmatism. Your choices include:
- Prescription reading glasses. If you have no other vision problems, you can use glasses with prescription lenses for reading only. You will need to remove these when you're not reading.
- Bifocals. These lenses have a visible horizontal line that separates your distance prescription, above the line, and your reading prescription, below the line.
- Trifocals. These glasses have corrections for close-up work, middle distance vision — such as for computer screens — and distance vision. Trifocals come with two visible horizontal lines in the lenses.
- Progressive multifocals. This type of lens has no visible horizontal lines, but has multiple powers for distance, middle distance and close-up corrections. Different areas of the lens have different focusing strengths.
- Office progressives. These lenses have corrections for computer-distance and close work. You generally use these at a computer or for reading and remove them for driving or walking around.
Contact lenses
People who don't want to wear eyeglasses often try contact lenses to improve their vision problems caused by presbyopia. This option may not work for you if you have certain conditions related to your eyelids, tear ducts or the surfaces of your eyes such as dry eye.
Several lens types are available:
- Bifocal contact lenses. Bifocal contact lenses provide distance and close-up correction on each contact. In one type of bifocal lens, the bottom, reading portion of the lens is weighted to keep the lens correctly positioned on your eye. Newer types of bifocal contact lenses offer one type of correction through the edges (periphery) of each lens and the other type of correction through the center of the lenses.
- Monovision contact lenses. With monovision contacts, you wear a contact lens for distance vision in one eye (usually your dominant eye) and a contact lens for close-up vision in the other eye.
- Modified monovision. With this option, you wear a bifocal or multifocal contact lens in one eye and a contact lens set for distance in the other (usually your dominant eye). You use both eyes for distance and one eye for reading.
Refractive surgery
Refractive surgery changes the shape of your cornea. For presbyopia, this treatment can be used to improve close-up vision in your nondominant eye. It's like wearing monovision contact lenses. Even after surgery, you may need to use eyeglasses for close-up work.
Talk with your doctor about the possible side effects, as this procedure is not reversible. You might want to try monovision contact lenses for a while before you commit to surgery.
Refractive surgical procedures include:
- Conductive keratoplasty. This procedure uses radiofrequency energy to apply heat to tiny spots around the cornea. The heat causes the edge of the cornea to shrink slightly, increasing its curve (steepness) and focusing ability. The results of conductive keratoplasty are variable and may not be long lasting.
-
Laser-assisted in situ keratomileusis (LASIK). With this procedure, your eye surgeon makes a thin, hinged flap deeper into your cornea. He or she then uses a laser to remove inner layers of your cornea to steepen its domed shape.
Recovery from LASIK surgery is usually more rapid and less painful than other corneal surgeries.
- Laser-assisted subepithelial keratectomy (LASEK). The surgeon creates an ultra-thin flap only in the cornea's outer protective cover (epithelium). He or she then uses a laser to reshape the cornea's outer layers, steepening its curve, and then replaces the epithelium.
- Photorefractive keratectomy (PRK). This procedure is similar to LASEK, except the surgeon completely removes the epithelium, then uses the laser to reshape the cornea. The epithelium is not replaced, but will grow back naturally, conforming to your cornea's new shape.
Lens implants
Some ophthalmologists use a procedure in which they remove the lens in each eye and replace it with a synthetic lens. This is called an intraocular lens.
Several types of lens implants are available for correcting presbyopia. Some allow your eye to see things both near and at a distance. Some change position or shape within the eye (accommodative lens). But lens implants can cause a decrease in the quality of your near vision, and you may still need reading glasses.
Possible side effects include glare and blurring. In addition, this surgery carries with it the same risks as those associated with cataract surgery, such as inflammation, infection, bleeding and glaucoma.
Corneal inlays
Some people have had success with a presbyopia treatment that involves inserting a small plastic ring with a central opening, into the cornea of one eye. The opening acts like a pinhole camera and allows in focused light so that you can see close objects.
If you don't like the results of your corneal inlay procedure, your eye surgeon can remove the rings, leaving you free to consider other treatment options.
Lifestyle and home remedies
You can't prevent presbyopia. You can help protect your eyes and your vision by following these tips:
- Have your eyes checked. Do this regularly even if you see well.
- Control chronic health conditions. Certain conditions, such as diabetes and high blood pressure, can affect your vision if you don't receive proper treatment.
- Protect your eyes from the sun. Wear glasses or sunglasses that block ultraviolet (UV) radiation. This is especially important if you spend long hours in the sun or are taking a prescription medication that increases your sensitivity to UV radiation.
- Prevent eye injuries. Wear protective eyewear when doing certain things, such as playing sports, mowing the lawn, or painting or using other products with toxic fumes. Nonprescription reading glasses generally don't provide safety protection.
- Eat healthy foods. Try to eat plenty of fruits, leafy greens and other vegetables. These foods generally contain high levels of antioxidants as well as vitamin A and beta carotene. They're also vital to maintaining healthy vision.
- Use the right glasses. The right glasses optimize your vision. Having regular exams will ensure that your eyeglass prescription is correct.
- Use good lighting. Turn up or add light for better vision.
- See your doctor immediately if you experience any of these symptoms — sudden loss of vision in one eye with or without pain, sudden hazy or blurred vision, double vision, or see flashes of light, black spots or halos around lights. Any of these symptoms may signal a serious medical or eye condition.
Preparing for an appointment
If you're having difficulty with your vision, start by seeing an eye specialist (optometrist or ophthalmologist). To make the most of your time with your doctor, it's a good idea to prepare for your appointment. Here's some information to help you prepare.
What you can do
- List symptoms you're experiencing, including any that may seem unrelated to the reason for which you scheduled the appointment.
- Make a list of all medications, vitamins and supplements you're taking.
- Consider taking along a family member or a friend who drives. You may not want to drive yourself home if your pupils have been dilated for the exam. And your companion can help remember information provided during your appointment.
- List questions to ask your doctor.
Preparing a list of questions can help you make the most of your time with your doctor. List your questions from most important to least important. For presbyopia, some basic questions to ask your doctor include:
- What's the most likely cause of my symptoms?
- Are there any other possible causes?
- Are the medications that I am taking causing these symptoms?
- Do I need any tests other than a complete eye examination?
- How often will I need eye exams?
- What treatments are available?
- What are the side effects or possible problems associated with each treatment?
- Which treatment would you recommend for me?
- What are the alternatives to the primary approach that you're suggesting?
- If I have other eye conditions, how can I best manage these conditions together?
- Are drugstore reading glasses safe to use?
- Do you have any brochures or other printed material I can take with me? What websites do you recommend?
In addition to the questions that you've prepared, don't hesitate to ask additional questions that may occur to you during your appointment.
What to expect from your doctor
Your doctor is likely to ask you a number of questions, including some that relate to your general health, your medical history, your eye health history, your family medical history and your history of eye problems. Your doctor may ask:
- When did you first begin experiencing symptoms?
- Have your symptoms been continuous or occasional?
- How severe are your symptoms?
- What, if anything, seems to improve your symptoms?
- What, if anything, appears to worsen your symptoms?
- Do you do a lot of reading or other close-up work?
What you can do in the meantime
Make sure you have adequate lighting. If you don't currently wear prescription eyeglasses, try a pair of over-the-counter (nonprescription) reading glasses.
Content Last Updated: September 30, 2020
Content provided by Mayo Clinic ©1998-2026 Mayo Foundation for Medical Education and Research (MFMER). All rights reserved. Terms of Use