Cleft lip and cleft palate
Overview
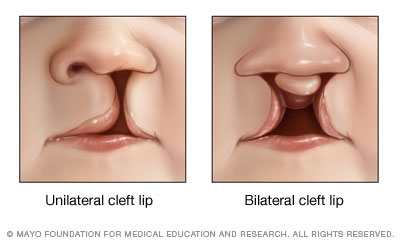
A cleft lip is an opening or split in the upper lip that occurs when developing facial structures in an unborn baby don't close completely. Cleft lip may be unilateral or bilateral. A baby with a cleft lip may also experience a cleft in the roof of the mouth (cleft palate).
Cleft lip and cleft palate are openings or splits in the upper lip, the roof of the mouth (palate) or both. Cleft lip and cleft palate result when facial structures that are developing in an unborn baby don't close completely.
Cleft lip and cleft palate are among the most common birth defects. They most commonly occur as isolated birth defects but are also associated with many inherited genetic conditions or syndromes.
Having a baby born with a cleft can be upsetting, but cleft lip and cleft palate can be corrected. In most babies, a series of surgeries can restore normal function and achieve a more normal appearance with minimal scarring.
Symptoms
Usually, a split (cleft) in the lip or palate is immediately identifiable at birth. Cleft lip and cleft palate may appear as:
- A split in the lip and roof of the mouth (palate) that affects one or both sides of the face
- A split in the lip that appears as only a small notch in the lip or extends from the lip through the upper gum and palate into the bottom of the nose
- A split in the roof of the mouth that doesn't affect the appearance of the face
Less commonly, a cleft occurs only in the muscles of the soft palate (submucous cleft palate), which are at the back of the mouth and covered by the mouth's lining. This type of cleft often goes unnoticed at birth and may not be diagnosed until later when signs develop. Signs and symptoms of submucous cleft palate may include:
- Difficulty with feedings
- Difficulty swallowing, with potential for liquids or foods to come out the nose
- Nasal speaking voice
- Chronic ear infections
When to see a doctor
A cleft lip and cleft palate are usually noticed at birth, and your doctor may start coordinating care at that time. If your baby has signs and symptoms of a submucous cleft palate, make an appointment with your child's doctor.
Causes
Cleft lip and cleft palate occur when tissues in the baby's face and mouth don't fuse properly. Normally, the tissues that make up the lip and palate fuse together in the second and third months of pregnancy. But in babies with cleft lip and cleft palate, the fusion never takes place or occurs only part way, leaving an opening (cleft).
Researchers believe that most cases of cleft lip and cleft palate are caused by an interaction of genetic and environmental factors. In many babies, a definite cause isn't discovered.
The mother or the father can pass on genes that cause clefting, either alone or as part of a genetic syndrome that includes a cleft lip or cleft palate as one of its signs. In some cases, babies inherit a gene that makes them more likely to develop a cleft, and then an environmental trigger actually causes the cleft to occur.
Risk factors
Several factors may increase the likelihood of a baby developing a cleft lip and cleft palate, including:
- Family history. Parents with a family history of cleft lip or cleft palate face a higher risk of having a baby with a cleft.
- Exposure to certain substances during pregnancy. Cleft lip and cleft palate may be more likely to occur in pregnant women who smoke cigarettes, drink alcohol or take certain medications.
- Having diabetes. There is some evidence that women diagnosed with diabetes before pregnancy may have an increased risk of having a baby with a cleft lip with or without a cleft palate.
- Being obese during pregnancy. There is some evidence that babies born to obese women may have increased risk of cleft lip and palate.
Males are more likely to have a cleft lip with or without cleft palate. Cleft palate without cleft lip is more common in females. In the United States, cleft lip and palate are reportedly most common in Native Americans and least common in African-Americans.
Complications
Children with cleft lip with or without cleft palate face a variety of challenges, depending on the type and severity of the cleft.
- Difficulty feeding. One of the most immediate concerns after birth is feeding. While most babies with cleft lip can breast-feed, a cleft palate may make sucking difficult.
- Ear infections and hearing loss. Babies with cleft palate are especially at risk of developing middle ear fluid and hearing loss.
- Dental problems. If the cleft extends through the upper gum, tooth development may be affected.
- Speech difficulties. Because the palate is used in forming sounds, the development of normal speech can be affected by a cleft palate. Speech may sound too nasal.
- Challenges of coping with a medical condition. Children with clefts may face social, emotional and behavioral problems due to differences in appearance and the stress of intensive medical care.
Prevention
After a baby is born with a cleft, parents are understandably concerned about the possibility of having another child with the same condition. While many cases of cleft lip and cleft palate can't be prevented, consider these steps to increase your understanding or lower your risk:
- Consider genetic counseling. If you have a family history of cleft lip and cleft palate, tell your doctor before you become pregnant. Your doctor may refer you to a genetic counselor who can help determine your risk of having children with cleft lip and cleft palate.
- Take prenatal vitamins. If you're planning to get pregnant soon, ask your doctor if you should take prenatal vitamins.
- Don't use tobacco or alcohol. Use of alcohol or tobacco during pregnancy increases the risk of having a baby with a birth defect.
Diagnosis
Most cases of cleft lip and cleft palate are noticed right away at birth and don't require special tests for diagnosis. Increasingly, cleft lip and cleft palate are seen on ultrasound before the baby is born.
Ultrasound before birth
A prenatal ultrasound is a test that uses sound waves to create pictures of the developing fetus. When analyzing the pictures, a doctor may detect a difference in the facial structures.
Cleft lip may be detected with ultrasound beginning around the 13th week of pregnancy. As the fetus continues developing, it may be easier to accurately diagnose a cleft lip. Cleft palate that occurs alone is more difficult to see using ultrasound.
If prenatal ultrasound shows a cleft, your doctor may offer a procedure to take a sample of amniotic fluid from your uterus (amniocentesis). The fluid test may indicate that the fetus has inherited a genetic syndrome that may cause other birth defects. However, most often the cause of cleft lip and cleft palate is unknown.
Treatment

Surgery to repair cleft lip creates a more normal lip appearance, structure and function. Surgery is done in a way to minimize the appearance of the scar. The scar will fade over time but will always be visible.
The goals of treatment for cleft lip and cleft palate are to improve the child's ability to eat, speak and hear normally and to achieve a normal facial appearance.
Care for children with cleft lip and cleft palate often involves a team of doctors and experts, including:
- Surgeons who specialize in cleft repair, such as plastic surgeons or ENTs
- Oral surgeons
- Ear, nose and throat doctors (ENTs, also called otorhinolaryngologists)
- Pediatricians
- Pediatric dentists
- Orthodontists
- Nurses
- Auditory or hearing specialists
- Speech therapists
- Genetic counselors
- Social workers
- Psychologists
Treatment involves surgery to repair the defect and therapies to improve any related conditions.
Surgery
Surgery to correct cleft lip and palate is based on your child's particular situation. Following the initial cleft repair, your doctor may recommend follow-up surgeries to improve speech or improve the appearance of the lip and nose.
Surgeries typically are performed in this order:
- Cleft lip repair — within the first 3 to 6 months of age
- Cleft palate repair — by the age of 12 months, or earlier if possible
- Follow-up surgeries — between age 2 and late teen years
Cleft lip and palate surgery takes place in a hospital. Your child will receive a general anesthetic, so he or she won't feel pain or be awake during surgery. Several different surgical techniques and procedures are used to repair cleft lip and palate, reconstruct the affected areas, and prevent or treat related complications.
In general, procedures may include:
- Cleft lip repair. To close the separation in the lip, the surgeon makes incisions on both sides of the cleft and creates flaps of tissue. The flaps are then stitched together, including the lip muscles. The repair should create a more normal lip appearance, structure and function. Initial nasal repair, if needed, is usually done at the same time.
- Cleft palate repair. Various procedures may be used to close the separation and rebuild the roof of the mouth (hard and soft palate), depending on your child's situation. The surgeon makes incisions on both sides of the cleft and repositions the tissue and muscles. The repair is then stitched closed.
- Ear tube surgery. For children with cleft palate, ear tubes may be placed to reduce the risk of chronic ear fluid, which can lead to hearing loss. Ear tube surgery involves placing tiny bobbin-shaped tubes in the eardrum to create an opening to prevent fluid buildup.
- Surgery to reconstruct appearance. Additional surgeries may be needed to improve the appearance of the mouth, lip and nose.
Surgery can significantly improve your child's appearance, quality of life, and ability to eat, breathe and talk. Possible risks of surgery include bleeding, infection, poor healing, widening or elevation of scars, and temporary or permanent damage to nerves, blood vessels or other structures.
Treatment for complications
Your doctor may recommend additional treatment for complications caused by cleft lip and cleft palate. Examples include:
- Feeding strategies, such as using a special bottle nipple or feeder
- Speech therapy to correct difficulty with speaking
- Orthodontic adjustments to the teeth and bite, such as having braces
- Monitoring by a pediatric dentist for tooth development and oral health from an early age
- Monitoring and treatment for ear infections, which may include ear tubes
- Hearing aids or other assistive devices for a child with hearing loss
- Therapy with a psychologist to help the child cope with the stress of repeated medical procedures or other concerns
Coping and support
No one expects to have a baby with a birth defect. When the excitement of new life is met with the stress of discovering that your baby has a cleft lip or cleft palate, the experience can be emotionally demanding for the entire family.
For parents and family
When welcoming a baby with cleft lip and cleft palate into your family, keep these coping tips in mind:
- Don't blame yourself. Focus your energy on supporting and helping your child.
- Acknowledge your emotions. It's completely normal to feel sad, overwhelmed and upset.
- Find support. Your hospital social worker can help you find community and financial resources and education.
For your child
You can support your child in many ways:
- Focus on your child as a person, not on the cleft.
- Point out positive qualities in others that don't involve physical appearance.
- Help your child gain confidence by allowing him or her to make decisions.
- Encourage confident body language, such as smiling and holding the head up with shoulders back.
- Keep the lines of communication open. If teasing or self-esteem issues arise at school, this can help your child feel safe in talking with you about it, so you can help address these issues.
Preparing for an appointment
If your child was diagnosed with cleft lip, cleft palate or both, you'll be referred to specialists who can help create a treatment plan for your child. Here's some information to help you get ready and what to expect from your doctor.
What you can do
Before your appointment:
- Find out any pre-appointment restrictions. At the time you make the appointment, ask if there's anything you need to do in advance, such as restrict your baby's diet.
- Make a list of any signs or symptoms your baby is experiencing, including any that may seem unrelated to the reason for the appointment.
- Consider taking a family member or friend along. Sometimes it can be difficult to remember all the information provided during an appointment. Someone who accompanies you may remember something that you missed or forgot.
- Make a list of questions to ask your doctor. List your questions from most important to least important in case time runs out.
Some questions to ask your doctor may include:
- Does my baby have a cleft lip, cleft palate or both?
- What caused my baby's cleft lip or cleft palate?
- What tests does my baby need?
- What is the best treatment plan?
- What are the alternatives to the treatment approach that you're suggesting?
- Are there any restrictions that my baby needs to follow?
- Should my baby see a specialist?
- Are there brochures or other printed material that I can have? What websites do you recommend?
- If I choose to have more children, is there a chance they may also have cleft lip or cleft palate?
Don't hesitate to ask other questions.
What to expect from your doctor
Your doctor is likely to ask you a number of questions, such as:
- Does your family have a history of cleft lip and cleft palate?
- Does your baby have problems while feeding, such as gagging or having milk come back up through the nose?
- Does your baby experience any symptoms that worry you?
- What, if anything, seems to improve your baby's symptoms?
- What, if anything, appears to worsen your baby's symptoms?
Preparing and anticipating questions will help you make the most of your appointment time and allow you to cover other points you want to address.
Content Last Updated: May 22, 2018
Content provided by Mayo Clinic ©1998-2026 Mayo Foundation for Medical Education and Research (MFMER). All rights reserved. Terms of Use