Prolactinoma
Overview
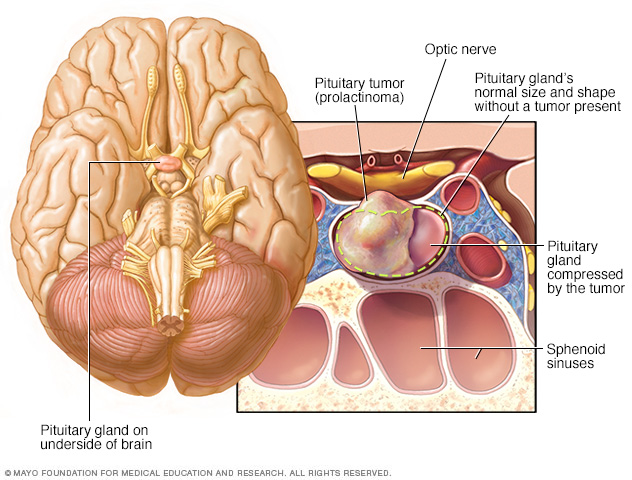
A prolactinoma is a type of tumor that develops in the pituitary gland at the base of your brain.
Prolactinoma is a noncancerous tumor of the pituitary gland. This tumor causes the pituitary to make too much of a hormone called prolactin. The major effect of prolactinoma is decreased levels of some sex hormones — estrogen in women and testosterone in men.
Although prolactinoma isn't life-threatening, it can cause vision difficulties, infertility and other problems. Prolactinoma is the most common type of hormone-producing tumor that can develop in your pituitary gland.
Doctors can often treat prolactinoma with medications to restore your prolactin level to normal. Surgery to remove the pituitary tumor also might be an option.
Symptoms
Prolactinoma might not cause any noticeable signs or symptoms. However, excessive prolactin in your blood (hyperprolactinemia) or pressure on surrounding tissues from a large tumor can cause signs or symptoms. Because elevated prolactin can disrupt the reproductive system (hypogonadism), some of the signs and symptoms of prolactinoma are specific to females or males.
In females, prolactinoma can cause:
- Irregular menstrual periods or no menstrual periods
- Milky discharge from the breasts when not pregnant or breast-feeding
- Painful intercourse due to vaginal dryness
- Acne and excessive body and facial hair growth
In males, prolactinoma can cause:
- Erectile dysfunction
- Decreased body and facial hair
- Enlarged breasts, uncommonly
In both sexes, prolactinoma can cause:
- Low bone density
- Reduction of other hormone production by the pituitary gland as a result of tumor pressure
- Loss of interest in sexual activity
- Headaches
- Visual disturbances
- Infertility
Women tend to notice signs and symptoms earlier than men do, when tumors are smaller in size, probably because of missed or irregular menstrual periods. Men tend to notice signs and symptoms later, when tumors are larger and more likely to cause headache or vision problems.
When to see a doctor
If you develop signs and symptoms associated with prolactinoma, see your doctor to determine the cause.
Causes
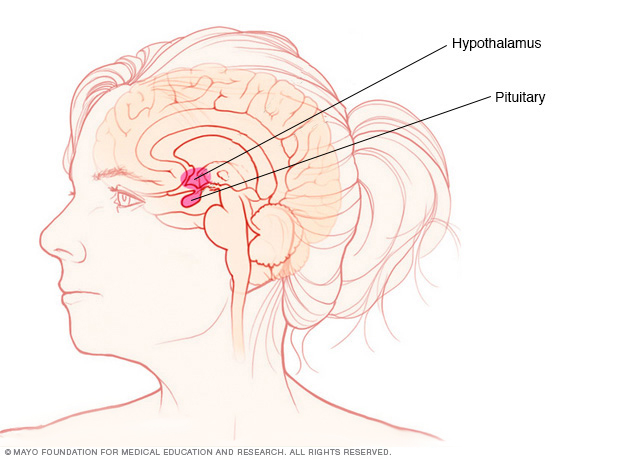
The pituitary gland and the hypothalamus are located within the brain and control hormone production.
Prolactinoma is one type of tumor that develops in the pituitary gland. The cause of these tumors is unknown.
The pituitary gland is a small bean-shaped gland situated at the base of your brain. Despite its small size, the pituitary gland influences nearly every part of your body. Its hormones help regulate important functions such as growth, metabolism, blood pressure and reproduction.
Other possible causes of prolactin overproduction include medications, other types of pituitary tumors, an underactive thyroid gland, ongoing irritation to the chest, pregnancy and breast-feeding.
Risk factors
More prolactinomas occur in women than men. The disorder is rare in children.
Complications
Complications of prolactinoma may include:
- Bone loss (osteoporosis). Too much prolactin can reduce production of the hormones estrogen and testosterone, resulting in decreased bone density and an increased risk of osteoporosis.
- Pregnancy complications. During a normal pregnancy, the production of estrogen increases. If you are pregnant and have a large prolactinoma, these high levels of estrogen may cause tumor growth and associated signs and symptoms, such as headaches and changes in vision.
- Vision loss. Left untreated, a prolactinoma may grow large enough to compress your optic nerve. This can cause a loss of peripheral vision.
- Low levels of other pituitary hormones. With larger prolactinomas, pressure on the normal pituitary gland can lead to lower levels of other hormones controlled by the pituitary, including thyroid hormones and cortisol (a stress-response hormone).
If you have prolactinoma and you want to become or are already pregnant, talk to your doctor. Adjustments in your treatment and monitoring may be necessary.
Diagnosis
If you have signs and symptoms that suggest you have prolactinoma, your doctor may recommend:
- Blood tests. Blood tests can detect the overproduction of prolactin and whether levels of other hormones controlled by the pituitary are within the normal range. Women of childbearing age also will have a pregnancy test.
- Brain imaging. Your doctor may be able to detect a pituitary tumor on an image generated by a magnetic resonance imaging scan of your brain.
- Vision tests. These can determine if a pituitary tumor has impaired your sight.
In addition, your doctor may refer you for more extensive testing with a doctor who specializes in treating disorders of the endocrine system (endocrinologist).
Treatment
Goals in the treatment of prolactinoma include:
- Return the production of prolactin to normal levels
- Restore normal pituitary gland function
- Reduce the size of the pituitary tumor
- Eliminate any signs or symptoms from tumor pressure, such as headaches or vision problems
- Improve quality of life
Prolactinoma treatment consists of two main therapies: medications and surgery.
Medications
Oral medications often can decrease the production of prolactin and eliminate symptoms. Medications may also shrink the tumor. However, long-term treatment with medications is generally necessary.
Doctors use drugs known as dopamine agonists to treat prolactinoma. These drugs mimic the effects of dopamine — the brain chemical that normally controls prolactin production. Commonly prescribed medications include bromocriptine (Cycloset, Parlodel) and cabergoline. These drugs decrease prolactin production and may shrink the tumor in most people with prolactinoma.
Common side effects
Nausea and vomiting, nasal stuffiness, headache, and drowsiness are common side effects of these medications. However, these side effects often can be minimized if your doctor starts you with a very low dose of medication and gradually increases the dose.
There have been rare cases of heart valve damage with cabergoline, but it's usually in people taking much higher doses for Parkinson's disease. Some people may develop compulsive behaviors, such as gambling, while taking these medications.
If medication shrinks the tumor significantly and your prolactin level remains normal for two years, you may be able to taper off the medication with your doctor's guidance. However, recurrence is common. Don't stop taking your medication without your doctor's approval.
Medication during pregnancy
Bromocriptine is more commonly prescribed when treating women who want to restore their fertility. However, once you become pregnant, your doctor will likely advise you to stop taking either medication.
Although both drugs are considered safe in early pregnancy, their safety throughout pregnancy isn't known. However, if you have a large prolactinoma or you develop signs and symptoms such as headaches or vision changes, your doctor may recommend that you restart your medication to prevent complications from prolactinoma.
If you're being treated for prolactinoma and you'd like to start a family, it's best to discuss your options with your doctor before you become pregnant.
Surgery
Surgery to remove the tumor is generally an option if drug therapy for prolactinoma doesn't work or you can't tolerate the medication. Surgery may be necessary to relieve pressure on the nerves that control your vision.
The type of surgery you have will depend largely on the size and extent of your tumor:
- Nasal surgery. Most people who need surgery have a procedure in which the tumor is removed through the nasal cavity. It's called transsphenoidal surgery. Complication rates are low because no other areas of the brain are touched during surgery, and this surgery leaves no visible scars.
- Transcranial surgery. If your tumor is large or has spread to nearby brain tissue, you may need this procedure, also known as a craniotomy. The surgeon removes the tumor through the upper part of the skull.
The outcome of surgery depends on the size and location of the tumor and your prolactin levels before surgery, as well as the skill of the surgeon. The higher the prolactin level, the slimmer the chance that prolactin production will return to normal after surgery.
Surgery corrects the prolactin level in most people with small pituitary tumors. However, many pituitary tumors come back within five years of surgery. For people with larger tumors that can only be partially removed, drug therapy often can return the prolactin level to a normal range after surgery.
Radiation
For people who don't respond to medication and aren't candidates for surgery, radiation therapy may be an option.
Preparing for an appointment
You'll likely start by seeing your family doctor. You may then be referred to a doctor who specializes in disorders that affect your glands and hormones (endocrinologist).
Here's some information to help you get ready for your appointment.
What you can do
- Write down your symptoms, including any that may seem unrelated to the reason for which you scheduled the appointment.
- For women, write down your menstrual history, age at onset of periods, episodes of missed menstrual periods, approximate dates and type of contraceptives used.
- Write down key personal information, including major stresses or recent life changes.
- List all medications, vitamins and supplements you're taking.
- Write down questions for your doctor.
Preparing a list of questions can help you make the most of your time with your doctor. For prolactinoma, some basic questions to ask include:
- What's the most likely cause of my symptoms?
- What are other possible causes?
- What tests do I need? Do they require special preparation?
- What treatments are available, and which do you recommend?
- What side effects can I expect from treatment?
- If I have surgery, will the prolactinoma come back?
- I have other health conditions. How can I best manage them together?
- Will I be able to have children?
- Is there a generic alternative to the medicine you're prescribing?
- Are there brochures or other printed material that I can take? What websites do you recommend?
Don't hesitate to ask any other questions.
What to expect from your doctor
Your doctor is likely to ask you questions, including:
- When did your symptoms begin?
- Have your symptoms been continuous or occasional?
- Does anything seem to improve your symptoms?
- What, if anything, appears to worsen your symptoms?
- Have you or family members ever had high calcium levels, kidney stones or tumors in endocrine glands?
Content Last Updated: May 28, 2020
Content provided by Mayo Clinic ©1998-2026 Mayo Foundation for Medical Education and Research (MFMER). All rights reserved. Terms of Use