Sleep apnea
Overview
Sleep apnea is a potentially serious sleep disorder in which breathing repeatedly stops and starts. If you snore loudly and feel tired even after a full night's sleep, you might have sleep apnea.
The main types of sleep apnea are:
- Obstructive sleep apnea, the more common form that occurs when throat muscles relax
- Central sleep apnea, which occurs when your brain doesn't send proper signals to the muscles that control breathing
- Complex sleep apnea syndrome, also known as treatment-emergent central sleep apnea, which occurs when someone has both obstructive sleep apnea and central sleep apnea
If you think you might have sleep apnea, see your doctor. Treatment can ease your symptoms and might help prevent heart problems and other complications.
Symptoms
The signs and symptoms of obstructive and central sleep apneas overlap, sometimes making it difficult to determine which type you have. The most common signs and symptoms of obstructive and central sleep apneas include:
- Loud snoring
- Episodes in which you stop breathing during sleep — which would be reported by another person
- Gasping for air during sleep
- Awakening with a dry mouth
- Morning headache
- Difficulty staying asleep (insomnia)
- Excessive daytime sleepiness (hypersomnia)
- Difficulty paying attention while awake
- Irritability
When to see a doctor
Loud snoring can indicate a potentially serious problem, but not everyone who has sleep apnea snores. Talk to your doctor if you have signs or symptoms of sleep apnea. Ask your doctor about any sleep problem that leaves you fatigued, sleepy and irritable.
Causes
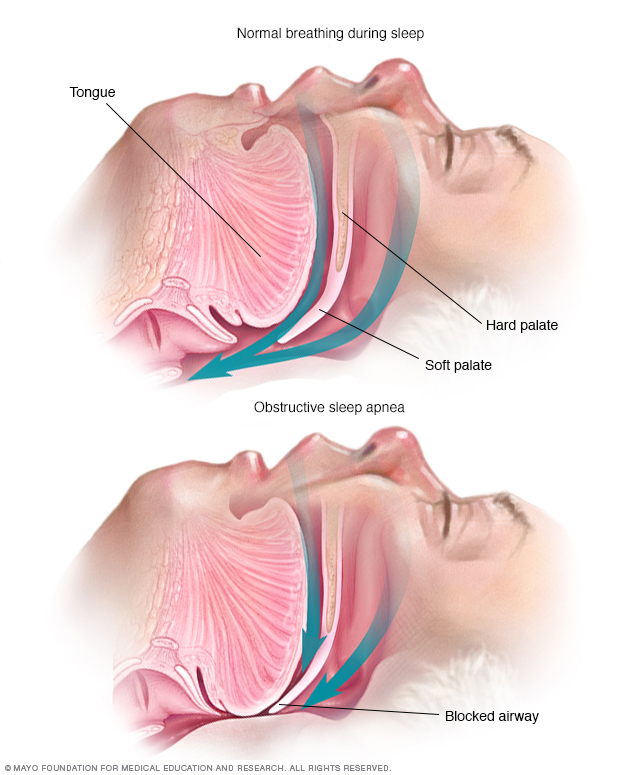
Obstructive sleep apnea occurs when the muscles that support the soft tissues in your throat, such as your tongue and soft palate, temporarily relax. When these muscles relax, your airway is narrowed or closed, and breathing is momentarily cut off.
Obstructive sleep apnea
This occurs when the muscles in the back of your throat relax. These muscles support the soft palate, the triangular piece of tissue hanging from the soft palate (uvula), the tonsils, the side walls of the throat and the tongue.
When the muscles relax, your airway narrows or closes as you breathe in. You can't get enough air, which can lower the oxygen level in your blood. Your brain senses your inability to breathe and briefly rouses you from sleep so that you can reopen your airway. This awakening is usually so brief that you don't remember it.
You might snort, choke or gasp. This pattern can repeat itself five to 30 times or more each hour, all night, impairing your ability to reach the deep, restful phases of sleep.
Central sleep apnea
This less common form of sleep apnea occurs when your brain fails to transmit signals to your breathing muscles. This means that you make no effort to breathe for a short period. You might awaken with shortness of breath or have a difficult time getting to sleep or staying asleep.
Risk factors
Sleep apnea can affect anyone, even children. But certain factors increase your risk.
Obstructive sleep apnea
Factors that increase the risk of this form of sleep apnea include:
- Excess weight. Obesity greatly increases the risk of sleep apnea. Fat deposits around your upper airway can obstruct your breathing.
- Neck circumference. People with thicker necks might have narrower airways.
- A narrowed airway. You might have inherited a narrow throat. Tonsils or adenoids also can enlarge and block the airway, particularly in children.
- Being male. Men are two to three times more likely to have sleep apnea than are women. However, women increase their risk if they're overweight, and their risk also appears to rise after menopause.
- Being older. Sleep apnea occurs significantly more often in older adults.
- Family history. Having family members with sleep apnea might increase your risk.
- Use of alcohol, sedatives or tranquilizers. These substances relax the muscles in your throat, which can worsen obstructive sleep apnea.
- Smoking. Smokers are three times more likely to have obstructive sleep apnea than are people who've never smoked. Smoking can increase the amount of inflammation and fluid retention in the upper airway.
- Nasal congestion. If you have difficulty breathing through your nose — whether from an anatomical problem or allergies — you're more likely to develop obstructive sleep apnea.
- Medical conditions. Congestive heart failure, high blood pressure, type 2 diabetes and Parkinson's disease are some of the conditions that may increase the risk of obstructive sleep apnea. Polycystic ovary syndrome, hormonal disorders, prior stroke and chronic lung diseases such as asthma also can increase risk.
Central sleep apnea
Risk factors for this form of sleep apnea include:
- Being older. Middle-aged and older people have a higher risk of central sleep apnea.
- Being male. Central sleep apnea is more common in men than it is in women.
- Heart disorders. Having congestive heart failure increases the risk.
- Using narcotic pain medications. Opioid medications, especially long-acting ones such as methadone, increase the risk of central sleep apnea.
- Stroke. Having had a stroke increases your risk of central sleep apnea or treatment-emergent central sleep apnea.
Complications
Sleep apnea is a serious medical condition. Complications can include:
-
Daytime fatigue. The repeated awakenings associated with sleep apnea make normal, restorative sleep impossible, making severe daytime drowsiness, fatigue and irritability likely.
You might have difficulty concentrating and find yourself falling asleep at work, while watching TV or even when driving. People with sleep apnea have an increased risk of motor vehicle and workplace accidents.
You might also feel quick-tempered, moody or depressed. Children and adolescents with sleep apnea might perform poorly in school or have behavior problems.
-
High blood pressure or heart problems. Sudden drops in blood oxygen levels that occur during sleep apnea increase blood pressure and strain the cardiovascular system. Having obstructive sleep apnea increases your risk of high blood pressure (hypertension).
Obstructive sleep apnea might also increase your risk of recurrent heart attack, stroke and abnormal heartbeats, such as atrial fibrillation. If you have heart disease, multiple episodes of low blood oxygen (hypoxia or hypoxemia) can lead to sudden death from an irregular heartbeat.
- Type 2 diabetes. Having sleep apnea increases your risk of developing insulin resistance and type 2 diabetes.
- Metabolic syndrome. This disorder, which includes high blood pressure, abnormal cholesterol levels, high blood sugar and an increased waist circumference, is linked to a higher risk of heart disease.
Complications with medications and surgery. Obstructive sleep apnea is also a concern with certain medications and general anesthesia. People with sleep apnea might be more likely to have complications after major surgery because they're prone to breathing problems, especially when sedated and lying on their backs.
Before you have surgery, tell your doctor about your sleep apnea and how it's being treated.
- Liver problems. People with sleep apnea are more likely to have abnormal results on liver function tests, and their livers are more likely to show signs of scarring (nonalcoholic fatty liver disease).
- Sleep-deprived partners. Loud snoring can keep anyone who sleeps near you from getting good rest. It's not uncommon for a partner to have to go to another room, or even to another floor of the house, to be able to sleep.
Diagnosis
Your doctor may make an evaluation based on your signs and symptoms and a sleep history, which you can provide with help from someone who shares your bed or your household, if possible.
You're likely to be referred to a sleep disorder center. There, a sleep specialist can help you determine your need for further evaluation.
An evaluation often involves overnight monitoring at a sleep center of your breathing and other body functions during sleep. Home sleep testing also might be an option. Tests to detect sleep apnea include:
- Nocturnal polysomnography. During this test, you're hooked up to equipment that monitors your heart, lung and brain activity, breathing patterns, arm and leg movements, and blood oxygen levels while you sleep.
-
Home sleep tests. Your doctor might provide you with simplified tests to be used at home to diagnose sleep apnea. These tests usually measure your heart rate, blood oxygen level, airflow and breathing patterns.
If the results are abnormal, your doctor might be able to prescribe a therapy without further testing. Portable monitoring devices don't detect all cases of sleep apnea, however, so your doctor might still recommend polysomnography even if your initial results are normal.
If you have obstructive sleep apnea, your doctor might refer you to an ear, nose and throat doctor to rule out blockage in your nose or throat. An evaluation by a heart doctor (cardiologist) or a doctor who specializes in the nervous system (neurologist) might be necessary to look for causes of central sleep apnea.
Treatment

To eliminate snoring and prevent sleep apnea, your doctor may recommend a device called a continuous positive airway pressure (CPAP) machine. A CPAP machine delivers just enough air pressure to a mask to keep your upper airway passages open, preventing snoring and sleep apnea.
For milder cases of sleep apnea, your doctor may recommend only lifestyle changes, such as losing weight or quitting smoking. If you have nasal allergies, your doctor will recommend treatment for your allergies.
If these measures don't improve your signs and symptoms or if your apnea is moderate to severe, a number of other treatments are available.
Certain devices can help open up a blocked airway. In other cases, surgery might be necessary.
Therapies
-
Continuous positive airway pressure (CPAP). If you have moderate to severe sleep apnea, you might benefit from using a machine that delivers air pressure through a mask while you sleep. With CPAP (SEE-pap), the air pressure is somewhat greater than that of the surrounding air and is just enough to keep your upper airway passages open, preventing apnea and snoring.
Although CPAP is the most common and reliable method of treating sleep apnea, some people find it cumbersome or uncomfortable. Some people give up on the CPAP machine, but with practice, most people learn to adjust the tension of the straps on the mask to obtain a comfortable and secure fit.
You might need to try more than one type of mask to find one that's comfortable. Don't stop using the CPAP machine if you have problems. Check with your doctor to see what changes can be made to increase your comfort.
Additionally, contact your doctor if you're still snoring or begin snoring again despite treatment. If your weight changes, the pressure settings of the CPAP machine might need to be adjusted.
- Other airway pressure devices. If using a CPAP machine continues to be a problem for you, you might be able to use a different type of airway pressure device that automatically adjusts the pressure while you're sleeping (auto-CPAP). Units that supply bilevel positive airway pressure (BPAP) also are available. These provide more pressure when you inhale and less when you exhale.
-
Oral appliances. Another option is wearing an oral appliance designed to keep your throat open. CPAP is more reliably effective than oral appliances, but oral appliances might be easier to use. Some are designed to open your throat by bringing your jaw forward, which can sometimes relieve snoring and mild obstructive sleep apnea.
A number of devices are available from your dentist. You might need to try different devices before finding one that works for you.
Once you find the right fit, you'll need to follow up with your dentist repeatedly during the first year and then regularly after that to ensure that the fit is still good and to reassess your signs and symptoms.
- Treatment for associated medical problems. Possible causes of central sleep apnea include heart or neuromuscular disorders, and treating those conditions might help.
- Supplemental oxygen. Using supplemental oxygen while you sleep might help if you have central sleep apnea. Various forms of oxygen are available with devices to deliver oxygen to your lungs.
-
Adaptive servo-ventilation (ASV). This more recently approved airflow device learns your normal breathing pattern and stores the information in a built-in computer. After you fall asleep, the machine uses pressure to normalize your breathing pattern and prevent pauses in your breathing.
ASV appears to be more successful than other forms of positive airway pressure at treating complex sleep apnea in some people. However, it might not be a good choice for people with predominant central sleep apnea and advanced heart failure.
You'll likely read, hear or see TV ads about different treatments for sleep apnea. Talk with your doctor about any treatment before you try it.
Surgery
Surgery is usually only an option after other treatments have failed. Generally, at least a three-month trial of other treatment options is suggested before considering surgery. However, for a small number of people with certain jaw structure problems, it's a good first option.
Surgical options might include:
-
Tissue removal. During this procedure (uvulopalatopharyngoplasty), your doctor removes tissue from the rear of your mouth and top of your throat. Your tonsils and adenoids usually are removed as well.
This type of surgery might be successful in stopping throat structures from vibrating and causing snoring. It's less effective than CPAP and isn't considered a reliable treatment for obstructive sleep apnea.
Removing tissues in the back of your throat with radiofrequency energy (radiofrequency ablation) might be an option if you can't tolerate CPAP or oral appliances.
- Tissue shrinkage. Another option is to shrink the tissue at the rear of your mouth and the back of your throat using radiofrequency ablation. This procedure might be used for mild to moderate sleep apnea. One study found this to have effects similar to that of tissue removal, but with fewer surgical risks.
- Jaw repositioning. In this procedure, your jaw is moved forward from the remainder of your face bones. This enlarges the space behind the tongue and soft palate, making obstruction less likely. This procedure is known as maxillomandibular advancement.
- Implants. Soft rods, usually made of polyester or plastic, are surgically implanted into the soft palate after you've received local anesthetic. More research is needed to determine how well implants work.
- Nerve stimulation. This requires surgery to insert a stimulator for the nerve that controls tongue movement (hypoglossal nerve). The increased stimulation helps keep the tongue in a position that keeps the airway open. More research is needed.
-
Creating a new air passageway (tracheostomy). You may need this form of surgery if other treatments have failed and you have severe, life-threatening sleep apnea. In this procedure, your surgeon makes an opening in your neck and inserts a metal or plastic tube through which you breathe.
You keep the opening covered during the day. But at night you uncover it to allow air to pass in and out of your lungs, bypassing the blocked air passage in your throat.
Other types of surgery may help reduce snoring and contribute to the treatment of sleep apnea by clearing or enlarging air passages:
- Surgery to remove enlarged tonsils or adenoids
- Weight-loss (bariatric) surgery
Lifestyle and home remedies
In some cases, self-care might be a way for you to deal with obstructive sleep apnea and possibly central sleep apnea. Try these tips:
- Lose excess weight. Even a slight weight loss might help relieve constriction of your throat. In some cases, sleep apnea can resolve if you return to a healthy weight, but it can recur if you regain the weight.
- Exercise. Regular exercise can help ease the symptoms of obstructive sleep apnea even without weight loss. Try to get 30 minutes of moderate activity, such as a brisk walk, most days of the week.
- Avoid alcohol and certain medications such as tranquilizers and sleeping pills. These relax the muscles in the back of your throat, interfering with breathing.
- Sleep on your side or abdomen rather than on your back. Sleeping on your back can cause your tongue and soft palate to rest against the back of your throat and block your airway. To keep from rolling onto your back while you sleep, try attaching a tennis ball to the back of your pajama top. There are also commercial devices that vibrate when you roll onto your back in sleep.
- Don't smoke. If you're a smoker, look for resources to help you quit.
Preparing for an appointment
If you or your partner suspects that you have sleep apnea, contact your primary care doctor. In some cases, you might be referred immediately to a sleep specialist.
Here's some information to help you get ready for your appointment.
What you can do
When you make the appointment, ask if there's anything you need to do in advance, such as modify your diet or keep a sleep diary.
Make a list of:
- Your symptoms, including any that may seem unrelated to the reason for which you scheduled the appointment, and when they began
- Key personal information, including family history of a sleep disorder
- All medications, vitamins or supplements you take, including doses
- Questions to ask your doctor
Take a family member or friend along, if possible, to help you remember the information you receive. Because your bed partner might be more aware of your symptoms than you are, it may help to have him or her along.
For sleep apnea, some questions to ask your doctor include:
- What's the most likely cause of my symptoms?
- What tests do I need? Do these tests require special preparation?
- Is my condition likely temporary or long lasting?
- What treatments are available?
- Which treatment do you think would be best for me?
- I have other health conditions. How can I best manage these conditions together?
- Should I see a specialist?
- Are there brochures or other printed material that I can have? What websites do you recommend?
What to expect from your doctor
Your doctor is likely to ask you questions, including:
- Have your symptoms been continuous, or do they come and go?
- How severe are your symptoms?
- How does your partner describe your symptoms?
- Do you know if you stop breathing during sleep? If so, how many times a night?
- Is there anything that has helped your symptoms?
- Does anything make your symptoms worse, such as sleep position or alcohol consumption?
What you can do in the meantime
- Try to sleep on your side.
- Avoid alcohol for four to six hours before bed.
- Don't take drugs that make you sleepy.
- If you're drowsy, avoid driving.
Content Last Updated: July 28, 2020
Content provided by Mayo Clinic ©1998-2026 Mayo Foundation for Medical Education and Research (MFMER). All rights reserved. Terms of Use