Spina bifida
Overview
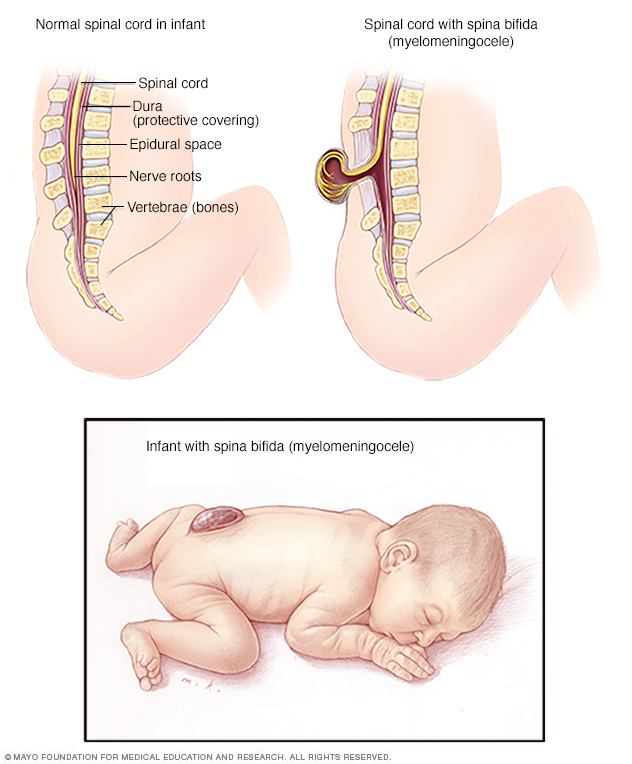
Myelomeningocele is a severe type of spina bifida in which the membranes and the spinal nerves protrude at birth, forming a sac on the baby's back. The exposed nervous system may become infected, so prompt surgery is needed after birth.
Spina bifida is a birth defect that occurs when the spine and spinal cord don't form properly. It's a type of neural tube defect. The neural tube is the structure in a developing embryo that eventually becomes the baby's brain, spinal cord and the tissues that enclose them.
Normally, the neural tube forms early in pregnancy and it closes by the 28th day after conception. In babies with spina bifida, a portion of the neural tube doesn't close or develop properly, causing defects in the spinal cord and in the bones of the spine.
Spina bifida can range from mild to severe, depending on the type of defect, size, location and complications. When necessary, early treatment for spina bifida involves surgery — although such treatment doesn't always completely resolve the problem.
Types
Spina bifida can occur in different types: spina bifida occulta, myelomeningocele (my-uh-lo-muh-NING-go-seel) or the very rare type meningocele (muh-NING-go-seel).
Spina bifida occulta
"Occulta" means hidden. It's the mildest and most common type. Spina bifida occulta results in a small separation or gap in one or more of the bones of the spine (vertebrae). Many people who have spina bifida occulta don't even know it, unless the condition is discovered during an imaging test done for unrelated reasons.
Myelomeningocele
Also known as open spina bifida, myelomeningocele is the most severe type. The spinal canal is open along several vertebrae in the lower or middle back. The membranes and spinal nerves push through this opening at birth, forming a sac on the baby's back, typically exposing tissues and nerves. This makes the baby prone to life-threatening infections and may also cause paralysis and bladder and bowel dysfunction.
Symptoms
Signs and symptoms of spina bifida vary by type and severity, and also between individuals.
- Spina bifida occulta. Typically there aren't any signs or symptoms because the spinal nerves aren't involved. But you can sometimes see signs on the newborn's skin above the spinal defect, including an abnormal tuft of hair, or a small dimple or birthmark. Sometimes, the skin marks can be signs of an underlying spinal cord issue that can be discovered with MRI or spinal ultrasound in a newborn.
- Myelomeningocele. In this severe type of spina bifida:
- The spinal canal remains open along several vertebrae in the lower or middle back
- Both the membranes and the spinal cord or nerves protrude at birth, forming a sac
- Tissues and nerves usually are exposed, though sometimes skin covers the sac
When to see a doctor
Typically, myelomeningocele is diagnosed before or right after birth, when medical care is available. These children should be followed by a specialized team of doctors throughout their lives, and families should be educated on the different complications to watch for.
Children with spina bifida occulta typically don't have any symptoms or complications, so usually only routine pediatric care is needed.
Causes
Doctors aren't certain what causes spina bifida. It's thought to result from a combination of genetic, nutritional and environmental risk factors, such as a family history of neural tube defects and folate (vitamin B-9) deficiency.
Risk factors
Spina bifida is more common among whites and Hispanics, and females are affected more often than males. Although doctors and researchers don't know for sure why spina bifida occurs, they have identified some risk factors:
- Folate deficiency. Folate, the natural form of vitamin B-9, is important to the development of a healthy baby. The synthetic form, found in supplements and fortified foods, is called folic acid. A folate deficiency increases the risk of spina bifida and other neural tube defects.
- Family history of neural tube defects. Couples who've had one child with a neural tube defect have a slightly higher chance of having another baby with the same defect. That risk increases if two previous children have been affected by the condition. In addition, a woman who was born with a neural tube defect has a greater chance of giving birth to a child with spina bifida. However, most babies with spina bifida are born to parents with no known family history of the condition.
- Some medications. For example, anti-seizure medications, such as valproic acid (Depakene), seem to cause neural tube defects when taken during pregnancy. This might happen because they interfere with the body's ability to use folate and folic acid.
- Diabetes. Women with diabetes who don't have well-controlled blood sugar have a higher risk of having a baby with spina bifida.
- Obesity. Pre-pregnancy obesity is associated with an increased risk of neural tube birth defects, including spina bifida.
- Increased body temperature. Some evidence suggests that increased body temperature (hyperthermia) in the early weeks of pregnancy may increase the risk of spina bifida. Elevating your core body temperature, due to fever or using a sauna or hot tub, has been associated with a possible slightly increased risk of spina bifida.
If you have known risk factors for spina bifida, talk with your doctor to determine if you need a larger dose or prescription dose of folic acid, even before a pregnancy begins.
If you take medications, tell your doctor. If you plan ahead, some medications can be adjusted to diminish the potential risk of spina bifida.
Complications
Spina bifida may cause minimal symptoms or minor physical disabilities. But severe spina bifida can lead to more significant physical disabilities. Severity is affected by:
- The size and location of the neural tube defect
- Whether skin covers the affected area
- Which spinal nerves come out of the affected area of the spinal cord
This list of possible complications may seem overwhelming, but not all children with spina bifida get all of these complications. And these conditions can be treated.
- Walking and mobility problems. The nerves that control the leg muscles don't work properly below the area of the spina bifida defect. This can cause muscle weakness of the legs and sometimes paralysis. Whether a child can walk typically depends on where the defect is, its size, and the care received before and after birth.
- Orthopedic complications. Children with myelomeningocele can have a variety of problems in the legs and spine because of weak muscles in the legs and back. The types of problems depend on the location of the defect. Possible problems include orthopedic issues such as:
- Curved spine (scoliosis)
- Abnormal growth
- Dislocation of the hip
- Bone and joint deformities
- Muscle contractures
- Bowel and bladder problems. Nerves that supply the bladder and bowels usually don't work properly when children have myelomeningocele. This is because the nerves that supply the bowel and bladder come from the lowest level of the spinal cord.
- Accumulation of fluid in the brain (hydrocephalus). Babies born with myelomeningocele commonly experience accumulation of fluid in the brain, a condition known as hydrocephalus.
- Shunt malfunction. Shunts placed in the brain to treat hydrocephalus can stop working or become infected. Warning signs may vary. Some of the warning signs of a shunt that isn't working include:
- Headaches
- Vomiting
- Sleepiness
- Irritability
- Swelling or redness along the shunt
- Confusion
- Changes in the eyes (fixed downward gaze)
- Trouble feeding
- Seizures
- Chiari malformation type II. Chiari malformation (kee-AH-ree mal-for-MAY-shun) type II is a common brain abnormality in children with the myelomeningocele type of spina bifida. The brainstem, or lowest part of the brain above the spinal cord, is elongated and positioned lower than usual. This can cause problems with breathing and swallowing. Rarely, compression on this area of the brain occurs and surgery is needed to relieve the pressure.
- Infection in the tissues surrounding the brain (meningitis). Some babies with myelomeningocele may develop meningitis, an infection in the tissues surrounding the brain. This potentially life-threatening infection may cause brain injury.
- Tethered spinal cord. Tethered spinal cord results when the spinal nerves bind to the scar where the defect was closed surgically. The spinal cord is less able to grow as the child grows. This progressive tethering can cause loss of muscle function to the legs, bowel or bladder. Surgery can limit the degree of disability.
- Sleep-disordered breathing. Both children and adults with spina bifida, particularly myelomeningocele, may have sleep apnea or other sleep disorders. Assessment for a sleep disorder in those with myelomeningocele helps detect sleep-disordered breathing, such as sleep apnea, which warrants treatment to improve health and quality of life.
- Skin problems. Children with spina bifida may get wounds on their feet, legs, buttocks or back. They can't feel when they get a blister or sore. Sores or blisters can turn into deep wounds or foot infections that are hard to treat. Children with myelomeningocele have a higher risk of wound problems in casts.
- Latex allergy. Children with spina bifida have a higher risk of latex allergy, an allergic reaction to natural rubber or latex products. Latex allergy may cause rash, sneezing, itching, watery eyes and a runny nose. It can also cause anaphylaxis, a potentially life-threatening condition in which swelling of the face and airways can make breathing difficult. So it's best to use latex-free gloves and equipment at delivery time and when caring for a child with spina bifida.
- Other complications. More problems may arise as children with spina bifida get older, such as urinary tract infections, gastrointestinal (GI) disorders and depression. Children with myelomeningocele may develop learning disabilities, such as problems paying attention, and difficulty learning reading and math.
Prevention
Folic acid, taken in supplement form starting at least one month before conception and continuing through the first trimester of pregnancy, greatly reduces the risk of spina bifida and other neural tube defects.
Get folic acid first
Having enough folic acid in your system by the early weeks of pregnancy is critical to prevent spina bifida. Because many women don't discover that they're pregnant until this time, experts recommend that all adult women of childbearing age take a daily supplement of 400 to 1,000 micrograms (mcg) of folic acid.
Several foods are fortified with 400 mcg of folic acid per serving, including:
- Enriched bread
- Pasta
- Rice
- Some breakfast cereals
Folic acid may be listed on food packages as folate, which is the natural form of folic acid found in foods.
Planning pregnancy
Adult women who are planning pregnancy or who could become pregnant should be advised to get 400 to 800 mcg of folic acid a day.
Your body doesn't absorb folate as easily as it absorbs synthetic folic acid, and most people don't get the recommended amount of folate through diet alone, so vitamin supplements are necessary to prevent spina bifida. And it's possible that folic acid will also help reduce the risk of other birth defects, including cleft lip, cleft palate and some congenital heart defects.
It's also a good idea to eat a healthy diet, including foods rich in folate or enriched with folic acid. This vitamin is present naturally in many foods, including:
- Beans and peas
- Citrus fruits and juices
- Egg yolks
- Milk
- Avocados
- Dark green vegetables, such as broccoli and spinach
When higher doses are needed
If you have spina bifida or if you've previously given birth to a child with spina bifida, you'll need extra folic acid before you become pregnant. If you're taking anti-seizure medications or you have diabetes, you may also benefit from a higher dose of this B vitamin. Check with your doctor before taking additional folic acid supplements.
Diagnosis
If you're pregnant, you'll be offered prenatal screening tests to check for spina bifida and other birth defects. The tests aren't perfect. Some mothers who have positive blood tests have babies without spina bifida. Even if the results are negative, there's still a small chance that spina bifida is present. Talk to your doctor about prenatal testing, its risks and how you might handle the results.
Blood tests
Spina bifida can be screened with maternal blood tests, but typically the diagnosis is made with ultrasound.
- Maternal serum alpha-fetoprotein (MSAFP) test. For the MSAFP test, a sample of the mother's blood is drawn and tested for alpha-fetoprotein (AFP) — a protein produced by the baby. It's normal for a small amount of AFP to cross the placenta and enter the mother's bloodstream. But abnormally high levels of AFP suggest that the baby has a neural tube defect, such as spina bifida, though high levels of AFP don't always occur in spina bifida.
- Test to confirm high AFP levels. Varying levels of AFP can be caused by other factors — including a miscalculation in fetal age or multiple babies — so your doctor may order a follow-up blood test for confirmation. If the results are still high, you'll need further evaluation, including an ultrasound exam.
- Other blood tests. Your doctor may perform the MSAFP test with two or three other blood tests. These tests are commonly done with the MSAFP test, but their objective is to screen for other abnormalities, such as trisomy 21 (Down syndrome), not neural tube defects.
Ultrasound
Fetal ultrasound is the most accurate method to diagnose spina bifida in your baby before delivery. Ultrasound can be performed during the first trimester (11 to 14 weeks) and second trimester (18 to 22 weeks). Spina bifida can be accurately diagnosed during the second trimester ultrasound scan. Therefore, this examination is crucial to identify and rule out congenital anomalies such as spina bifida.
An advanced ultrasound also can detect signs of spina bifida, such as an open spine or particular features in your baby's brain that indicate spina bifida. In expert hands, ultrasound is also effective in assessing severity.
Amniocentesis
If the prenatal ultrasound confirms the diagnosis of spina bifida, your doctor may request amniocentesis. During amniocentesis, your doctor uses a needle to remove a sample of fluid from the amniotic sac that surrounds the baby.
This examination may be important to rule out genetic diseases, despite the fact that spina bifida is rarely associated with genetic diseases.
Discuss the risks of amniocentesis, including a slight risk of loss of the pregnancy, with your doctor.
Treatment
Spina bifida treatment depends on the severity of the condition. Spina bifida occulta often doesn't require any treatment at all, but other types of spina bifida do.
Surgery before birth
Nerve function in babies with spina bifida can worsen after birth if spina bifida isn't treated. Prenatal surgery for spina bifida (fetal surgery) takes place before the 26th week of pregnancy. Surgeons expose the pregnant mother's uterus surgically, open the uterus and repair the baby's spinal cord. In select patients, this procedure can also be performed less invasively with a fetoscope through ports in the uterus.
Research suggests that children with spina bifida who had fetal surgery may have reduced disability and be less likely to need crutches or other walking devices. Fetal surgery may also reduce the risk of hydrocephalus. Ask your doctor whether this procedure may be appropriate for you. Discuss the potential benefits and risks, such as possible premature delivery and other complications, for you and your baby.
It's important to have a comprehensive evaluation to determine whether fetal surgery is feasible. This specialized surgery should only be done at a health care facility that has experienced fetal surgery experts, a multispecialty team approach and neonatal intensive care. Typically the team includes a fetal surgeon, pediatric neurosurgeon, maternal-fetal medicine specialist, fetal cardiologist and neonatologist.
Cesarean birth
Many babies with myelomeningocele tend to be in a feet-first (breech) position. If your baby is in this position or if your doctor has detected a large cyst or sac, cesarean birth may be a safer way to deliver your baby.
Surgery after birth
Myelomeningocele requires surgery. Performing the surgery early can help minimize the risk of infection associated with the exposed nerves. It may also help protect the spinal cord from more trauma.
During the procedure, a neurosurgeon places the spinal cord and exposed tissue inside the baby's body and covers them with muscle and skin. At the same time, the neurosurgeon may place a shunt in the baby's brain to control hydrocephalus.
Treatment for complications
In babies with myelomeningocele, irreparable nerve damage has likely already occurred and ongoing care from a multispecialty team of surgeons, physicians and therapists is usually needed. Babies with myelomeningocele may need more surgery for a variety of complications. Treatment for complications — such as weak legs, bladder and bowel problems, or hydrocephalus — typically begins soon after birth.
Depending on the severity of spina bifida and the complications, treatment options may include:
- Walking and mobility aids. Some babies may start exercises to prepare their legs for walking with braces or crutches when they're older. Some children may need walkers or a wheelchair. Mobility aids, along with regular physical therapy, can help a child become independent. Even children who need a wheelchair can learn to function very well and become self-sufficient.
- Bowel and bladder management. Routine bowel and bladder evaluations and management plans help reduce the risk of organ damage and illness. Evaluations include X-rays, kidney scans, ultrasounds, blood tests and bladder function studies. These evaluations will be more frequent in the first few years of life but less often as children grow. A specialist in pediatric urology with experience in evaluating and performing surgery on children with spina bifida may offer the most effective management options.
- Bowel management may include oral medications, suppositories, enemas, surgery or a combination of these approaches.
- Bladder management may include medications, using catheters to empty the bladder, surgery or a combination of treatments.
- Surgery for hydrocephalus. Most babies with myelomeningocele will need a surgically placed tube that allows fluid in the brain to drain into the abdomen (ventricular shunt). This tube might be placed just after birth, during the surgery to close the sac on the lower back or later as fluid accumulates. A less invasive procedure, called endoscopic third ventriculostomy, may be an option. But candidates must be carefully chosen and meet certain criteria. During the procedure, the surgeon uses a small video camera to see inside the brain and makes a hole in the bottom of or between the ventricles so cerebrospinal fluid can flow out of the brain.
- Treatment and management of other complications. Special equipment such as bath chairs, commode chairs and standing frames may help with daily functioning. Whatever the issue — orthopedic complications, tethered spinal cord, GI issues, skin problems or others — most spina bifida complications can be treated or at least managed to improve quality of life.
Ongoing care
Children with spina bifida need close follow-up care and observation. Their primary care doctors evaluate growth, the need for vaccinations and general medical issues, and they coordinate medical care.
Children with spina bifida also often need treatment and ongoing care from:
- Physical medicine and rehabilitation
- Neurology
- Neurosurgery
- Urology
- Orthopedics
- Physical therapy
- Occupational therapy
- Special education teachers
- Social workers
- Dietitians
Parents and other caregivers are a key part of the team. They can learn how to help manage a child's condition and how to encourage and support the child emotionally and socially.
Coping and support
News that your newborn child has a condition such as spina bifida can naturally cause you to feel grief, anger, frustration, fear and sadness. There's good reason for hope, however, because most people with spina bifida live active, productive and full lives — especially with encouragement and support from loved ones. Children with spina bifida can go on to college, hold jobs and have families.
Special accommodations may be necessary along the way, but encourage your child to be as independent as possible.
Independent mobility is an important and appropriate goal for all children with spina bifida. This may mean walking with or without braces, using walking aids (such as canes or crutches), or exclusively using a wheelchair. Encouraging children to participate in activities with their peers can be beneficial, and caregivers can help adjust activities to accommodate physical limitations.
Many children with spina bifida have normal intelligence, but some may need educational intervention for learning problems. Some children experience difficulty with attention, concentration or language that requires treatment from professionals outside of school.
As for any child with a chronic medical condition, children with spina bifida may benefit from meeting with mental health professionals, such as a child psychologist, to assist with adjustment and coping. Most children with spina bifida are resilient and adapt to their challenges with support from their parents, teachers and other caregivers.
If your child has spina bifida, you may benefit from finding a support group of other parents who are dealing with the condition. Talking with others who understand the challenges of living with spina bifida can be helpful.
Preparing for an appointment
Your doctor will likely suspect or diagnose your baby's condition during your pregnancy. If that's the case, you'll likely consult with a multispecialty team of physicians, surgeons and physical therapists at a center that specializes in spina bifida treatment.
Here's some information to help you get ready for your appointment and know what to expect from your health care providers if there are suspicions that your baby may have spina bifida.
What you can do
To prepare for the appointment:
- Be aware of any pre-appointment instructions. At the time you make the appointment, be sure to ask if there's anything you need to do in advance, such as drink extra water before an ultrasound.
- Make a list of all medications, vitamins, herbs and supplements that you took before and during your pregnancy, and the dosages.
- Ask a family member or friend to come with you, if possible. Sometimes it can be difficult to remember all the information provided to you during an appointment. Someone who accompanies you may remember something that you missed or forgot.
- Create a list of questions to ask your doctor, starting with the most important in case time runs out.
For spina bifida, some basic questions to ask include:
- Is spina bifida present and how severe is it?
- Is there evidence of water on the brain (hydrocephalus)?
- Can my baby be treated during pregnancy?
- What will be done for my baby immediately after birth?
- Will the treatment cure my child?
- Will there be any lasting effects?
- Who can I contact to find out about community resources that may be able to help my child?
- What is the likelihood of this happening again in future pregnancies?
- How can I keep this from happening again in the future?
- Are there any brochures or other printed material that I can have? What websites do you recommend?
In addition to the questions that you've prepared, don't hesitate to ask other questions during your appointment.
What to expect from your doctor
Being ready to answer questions from your doctor may reserve time to go over any points you want to focus on. Your doctor may ask, for example:
- Have you ever had a child with spina bifida or other birth defects?
- Is there a family history of spina bifida?
- Did you take folic acid (vitamin B-9) before and during your pregnancy?
- Are you taking any anti-seizure medications, or were you taking them at the beginning of your pregnancy?
- If necessary, are you able to travel to a facility that offers specialized care?
Content Last Updated: March 17, 2021
Content provided by Mayo Clinic ©1998-2026 Mayo Foundation for Medical Education and Research (MFMER). All rights reserved. Terms of Use