Ear tubes
Overview
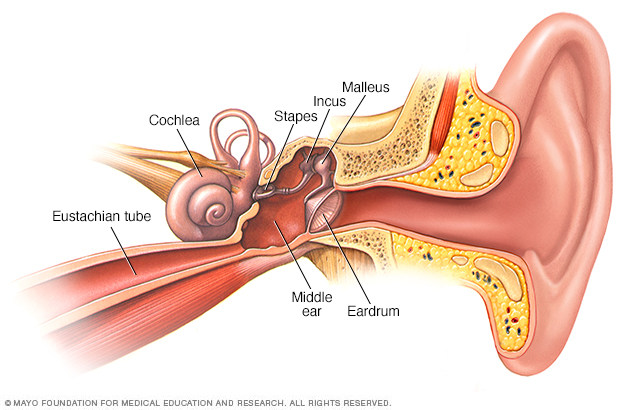
The middle ear includes three small bones — the hammer (malleus), anvil (incus) and stirrup (stapes). The middle ear is separated from your external ear by the eardrum and connected to the back of your nose and throat by a narrow passageway called the eustachian tube. The cochlea, a snail-shaped structure, is part of your inner ear.
Ear tubes are tiny, hollow cylinders that are surgically inserted into the eardrum. This opening enables drainage of the middle ear, allows air to flow into the middle ear and prevents the buildup of fluids behind the eardrum. An ear tube is usually made of metal or plastic.
Ear tubes are also called tympanostomy tubes, ventilation tubes, myringotomy tubes or pressure equalization tubes.
Ear tubes are often recommended for children who have persistent fluid buildup behind the eardrum, especially if the condition causes hearing loss or affects speech development. Your child's doctor may also recommend ear tubes if your child gets frequent ear infections.
Most ear tubes fall out within four to 18 months, and the holes heal shut on their own. Some tubes need to be removed, and some holes may need to be surgically closed.
Why it's done
An ear tube is used to treat and prevent the buildup of fluids in the middle ear.
The middle ear
The middle ear is the space behind the eardrum that contains three tiny vibrating bones. An opening in the middle ear leads to a tube that connects the middle ear to the back of the throat (eustachian tube). This tube performs three tasks:
- Equalizing air pressure in the middle ear
- Allowing fresh air into the middle ear
- Allowing fluids to drain from the middle ear and into the throat
In young children, the eustachian tube is short, floppy and mostly horizontal — factors that can lead to dysfunction or blockage of the tube.
Problems with the middle ear
Conditions that may be treated with ear tubes generally have two related features:
- Inflammation (otitis media)
- Buildup of fluids (effusion)
Ear tubes may be an appropriate treatment for the following conditions:
- Middle ear infection (acute otitis media) is caused by a bacterium or virus. The infection results in inflammation and fluids in the middle ear. Ear tubes may be used to prevent new infections. Your doctor may recommend them if your child has three or more distinct episodes of infection in six months or four or more episodes in a year.
- Otitis media with effusion is the buildup of fluids without signs or symptoms of infection. This may be caused by persistent fluids after an infection, problems with the eustachian tubes or another condition that prevents drainage. The fluids can cause both hearing loss and balance problems. Ear tubes are especially important if hearing problems result in delayed language development, other delays in learning, poor performance in school or behavior problems.
- Chronic middle ear infection is a bacterial infection that doesn't respond to antibiotic treatment. An ear tube may be inserted to drain the ear and allow for antibiotic drops directly into the middle ear.
- Chronic suppurative otitis media is ongoing inflammation of the middle ear that results in a tear in the eardrum and persistent discharge from the ear. It can be caused by infection, blockage of the eustachian tube or injury to the ear. An ear tube can allow drainage after the eardrum is surgically repaired and allow for direct ear drop treatment.
Risks
Ear tube placement is a relatively safe procedure with a low risk of serious complications. Possible risks include:
- Bleeding and infection
- Persistent fluid drainage
- Blocked tubes from blood, mucus or other secretions
- Scarring or weakening of the eardrum
- Tubes falling out too early or staying in too long
- Failure of the eardrum to close after the tube falls out or is removed
Anesthesia
Surgery for ear tube placement usually requires general anesthesia. Although the risks of anesthesia are very low in otherwise healthy children, possible problems include:
- Nausea or vomiting after the procedure
- Breathing difficulties
- Allergic reaction
- Irregular heartbeats
How you prepare
You'll receive instructions from the hospital on how to prepare your child for surgery to place ear tubes.
Information to provide may include:
- All medications your child takes regularly
- Your child's history or family history of adverse reactions to anesthesia
- Known allergy or other negative reactions to medications, such as antibiotics
Questions to ask your doctor or the hospital staff:
- When does my child need to start fasting?
- What drugs can he or she take before surgery?
- When should we arrive at the hospital?
- Where do we need to check in?
- What is the expected recovery time?
- How will the anesthesia be administered — with a face mask, injection or intravenous (IV) line?
Tips for helping your child prepare include the following:
- Start talking about the hospital visit a few days before the procedure.
- Explain that the procedure will help make his or her ears feel better or make it easier to hear.
- Explain that a special medicine will help him or her sleep during the surgery.
- Let your child pick out a favorite comfort toy, such as a blanket or stuffed animal, that you can take to the hospital.
- Explain that you will be there during the procedure.
What you can expect
Before the procedure
A surgeon specializing in ear, nose and throat disorders performs the surgery for placing ear tubes.
Anesthesia
The surgeon usually performs the procedure during general anesthesia, so your child isn't aware of anything during the procedure.
The surgical team places several monitors on your child's body to be sure heart rate, blood pressure and blood oxygen remain at safe levels throughout the procedure. These monitors include a blood pressure cuff on your child's arm and heart-monitor leads attached to your child's chest.
During the procedure
The procedure usually takes about 15 minutes. The surgeon:
- Makes a tiny hole (incision) in the eardrum (myringotomy) with a small scalpel or laser
- Suctions out fluids from the middle ear
- Inserts the tube in the hole in the eardrum
After the procedure
After surgery, your child is moved to a recovery room where the health care team watches for complications from the surgery and anesthesia. If there aren't any complications, your child will be able to go home within a few hours.
Your child will likely be sleepy and irritable for the rest of the day and possibly nauseous from the anesthesia. In most cases, children resume regular activities within 24 hours of the surgery.
Follow-up care
Your child's doctor will advise you about follow-up care after ear tube placement. If there are no complications, standard care includes the following:
- A follow-up appointment will be scheduled within two to four weeks of the procedure. At that time, your child's ear, nose and throat specialist (otolaryngologist) will check for appropriate placement and function of the tubes. Other follow-up appointments with the ear, nose and throat specialist or your child's primary care doctor will be scheduled every four to six months.
- Your child may be prescribed antibiotic eardrops to prevent infection after surgery. Use all the medication as directed even if there's no drainage or other signs of infection.
- If your child had hearing loss before the procedure, the doctor will also order a hearing test (audiogram) to evaluate hearing afterward.
- Your child likely won't need to wear earplugs while swimming or bathing unless his or her doctor suggests them.
When to contact your doctor
Reasons to see your child's ear, nose and throat specialist outside of regularly scheduled follow-up appointments include:
- Yellow, brown or bloody discharge from the ear that continues for more than a week
- Persistent pain, hearing problems or balance problems
Results
Ear tubes help restore ventilation and drainage of the ear. Ear tube placement often results in:
- Reduced risk of ear infections
- Restored or improved hearing
- Improved speech
- Improvements in behavior and sleep problems related to frequent or persistent ear infections
Even with ear tubes, your child may still get an occasional ear infection.
Usually, an ear tube stays in the eardrum for four to 18 months and then falls out on its own. Sometimes, a tube doesn't fall out and needs to be surgically removed. In some cases, the ear tube falls out too soon, and another needs to be put in the eardrum.
Content Last Updated: June 22, 2021
Content provided by Mayo Clinic ©1998-2026 Mayo Foundation for Medical Education and Research (MFMER). All rights reserved. Terms of Use