Tracheostomy
Overview
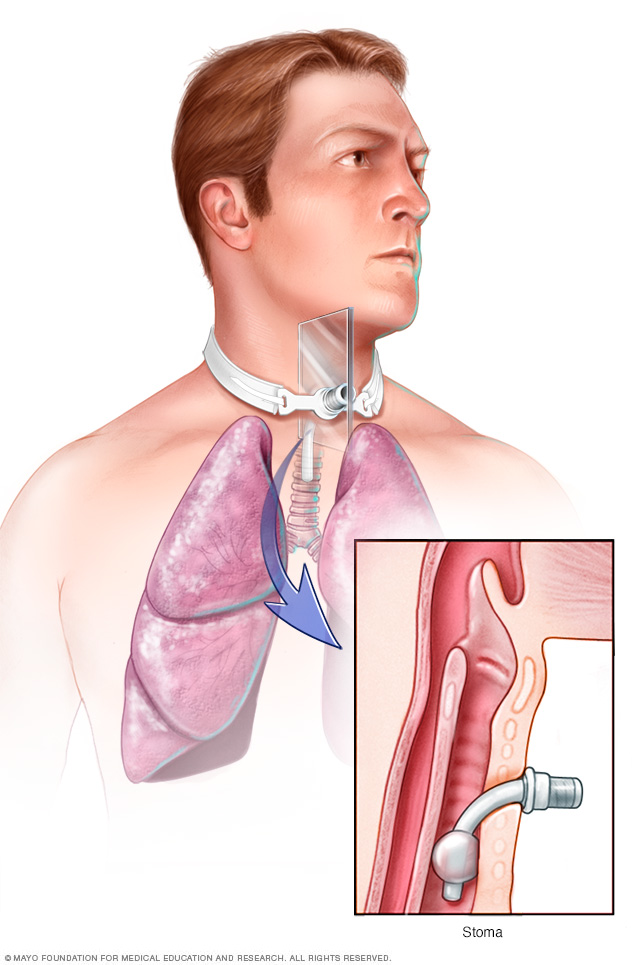
A tracheostomy is a surgically created hole (stoma) in your windpipe (trachea) that provides an alternative airway for breathing. A tracheostomy tube is inserted through the hole and secured in place with a strap around your neck.
Tracheostomy (tray-key-OS-tuh-me) is a hole that surgeons make through the front of the neck and into the windpipe (trachea). A tracheostomy tube is placed into the hole to keep it open for breathing. The term for the surgical procedure to create this opening is tracheotomy.
A tracheostomy provides an air passage to help you breathe when the usual route for breathing is somehow blocked or reduced. A tracheostomy is often needed when health problems require long-term use of a machine (ventilator) to help you breathe. In rare cases, an emergency tracheotomy is performed when the airway is suddenly blocked, such as after a traumatic injury to the face or neck.
When a tracheostomy is no longer needed, it's allowed to heal shut or is surgically closed. For some people, a tracheostomy is permanent.
Why it's done
Situations that may call for a tracheostomy include:
- Medical conditions that make it necessary to use a breathing machine (ventilator) for an extended period, usually more than one or two weeks
- Medical conditions that block or narrow your airway, such as vocal cord paralysis or throat cancer
- Paralysis, neurological problems or other conditions that make it difficult to cough up secretions from your throat and require direct suctioning of the windpipe (trachea) to clear your airway
- Preparation for major head or neck surgery to assist breathing during recovery
- Severe trauma to the head or neck that obstructs breathing
- Other emergency situations when breathing is obstructed and emergency personnel can't put a breathing tube through your mouth and into your trachea
Emergency care
Most tracheotomies are performed in a hospital setting. However, in the case of an emergency, it may be necessary to create a hole in a person's throat when outside of a hospital, such as at the scene of an accident.
Emergency tracheotomies are difficult to perform and have an increased risk of complications. A related and somewhat less risky procedure used in emergency care is a cricothyrotomy (kry-koe-thie-ROT-uh-me). This procedure creates a hole directly into the voice box (larynx) at a site immediately below the Adam's apple (thyroid cartilage).
Once a person is transferred to a hospital and stabilized, a cricothyrotomy is replaced by a tracheostomy if there's a need for long-term breathing assistance.
Risks
Tracheostomies are generally safe, but they do have risks. Some complications are particularly likely during or shortly after surgery. The risk of such problems greatly increases when the tracheotomy is performed as an emergency procedure.
Immediate complications include:
- Bleeding
- Damage to the trachea, thyroid gland or nerves in the neck
- Misplacement or displacement of the tracheostomy tube
- Air trapped in tissue under the skin of the neck (subcutaneous emphysema), which can cause breathing problems and damage to the trachea or food pipe (esophagus)
- Buildup of air between the chest wall and lungs (pneumothorax), which causes pain, breathing problems or lung collapse
- A collection of blood (hematoma), which may form in the neck and compress the trachea, causing breathing problems
Long-term complications are more likely the longer a tracheostomy is in place. These problems include:
- Obstruction of the tracheostomy tube
- Displacement of the tracheostomy tube from the trachea
- Damage, scarring or narrowing of the trachea
- Development of an abnormal passage between the trachea and the esophagus (tracheoesophageal fistula), which can increase the risk of fluids or food entering the lungs
- Development of a passage between the trachea and the large artery that supplies blood to the right arm and right side of the head and neck (tracheoinnominate fistula), which can result in life-threatening bleeding
- Infection around the tracheostomy or infection in the trachea and bronchial tubes (tracheobronchitis) and lungs (pneumonia)
If you still need a tracheostomy after you've left the hospital, you'll need to keep regularly scheduled appointments for monitoring possible complications. You'll also receive instructions about when you should call your doctor about problems, such as:
- Bleeding at the tracheostomy site or from the trachea
- Difficulty breathing through the tube
- Pain or a change in comfort level
- Redness or swelling around the tracheostomy
- A change in the position of your tracheostomy tube
How you prepare
How you prepare for a tracheostomy depends on the type of procedure you'll undergo. If you'll be receiving general anesthesia, your doctor may ask that you avoid eating and drinking for several hours before your procedure. You may also be asked to stop certain medications.
Plan for your hospital stay
After the tracheostomy procedure, you'll likely stay in the hospital for several days as your body heals. If possible, plan ahead for your hospital stay by bringing:
- Comfortable clothing, such as pajamas, a robe and slippers
- Personal care items, such as your toothbrush and shaving supplies
- Entertainment to help you pass the time, such as books, magazines or games
- A communication method, such as a pencil and a pad of paper, a smartphone, or a computer, as you'll be unable to talk at first
What you can expect
During the procedure
A tracheotomy is most commonly performed in an operating room with general anesthesia, which makes you unaware of the surgical procedure. A local anesthetic to numb the neck and throat is used if the surgeon is worried about the airway being compromised from general anesthesia or if the procedure is being done in a hospital room rather than an operating room.
The type of procedure you undergo depends on why you need a tracheostomy and whether the procedure was planned. There are essentially two options:
- Surgical tracheotomy can be performed in an operating room or in a hospital room. The surgeon usually makes a horizontal incision through the skin at the lower part of the front of your neck. The surrounding muscles are carefully pulled back and a small portion of the thyroid gland is cut, exposing the windpipe (trachea). At a specific spot on your windpipe near the base of your neck, the surgeon creates a tracheostomy hole.
- Minimally invasive tracheotomy (percutaneous tracheotomy) is typically performed in a hospital room. The doctor makes a small incision near the base of the front of the neck. A special lens is fed through the mouth so that the surgeon can view the inside of the throat. Using this view of the throat, the surgeon guides a needle into the windpipe to create the tracheostomy hole, then expands it to the appropriate size for the tube.
For both procedures, the surgeon inserts a tracheostomy tube into the hole. A neck strap attached to the face plate of the tube keeps it from slipping out of the hole, and temporary sutures can be used to secure the faceplate to the skin of your neck.
After the procedure
You'll likely spend several days in the hospital as your body heals. During that time, you'll learn skills necessary for maintaining and coping with your tracheostomy:
- Caring for your tracheostomy tube. A nurse will teach you how to clean and change your tracheostomy tube to help prevent infection and reduce the risk of complications. You'll continue to do this as long as you have a tracheostomy.
- Speaking. Generally, a tracheostomy prevents speaking because exhaled air goes out the tracheostomy opening rather than up through your voice box. But there are devices and techniques for redirecting airflow enough to produce speech. Depending on the type of tube, width of your trachea and condition of your voice box, you may be able to speak with the tube in place. If necessary, a speech therapist or a nurse trained in tracheostomy care can suggest options for communicating and help you learn to use your voice again.
- Eating. While you're healing, swallowing will be difficult. You'll receive nutrients through an intravenous (IV) line inserted into a vein in your body, a feeding tube that passes through your mouth or nose, or a tube inserted directly into your stomach. When you're ready to eat again, you may need to work with a speech therapist, who can help you regain the muscle strength and coordination needed for swallowing.
- Coping with dry air. The air you breathe will be much drier because it no longer passes through your moist nose and throat before reaching your lungs. This can cause irritation, coughing and excess mucus coming out of the tracheostomy. Putting small amounts of saline directly into the tracheostomy tube, as directed, may help loosen secretions. Or a saline nebulizer treatment may help. A device called a heat and moisture exchanger captures moisture from the air you exhale and humidifies the air you inhale. A humidifier or vaporizer adds moisture to the air in a room.
- Managing other effects. Your health care team will show you ways to care for other common effects related to having a tracheostomy. For example, you may learn to use a suction machine to help you clear secretions from your throat or airway.
Results
In most cases, a tracheostomy is temporary, providing an alternative breathing route until other medical issues are resolved. If you need to remain connected to a ventilator indefinitely, the tracheostomy is often the best permanent solution.
Your health care team will help you determine when it's appropriate to remove the tracheostomy tube. The hole may close and heal on its own, or it can be closed surgically.
Content Last Updated: October 22, 2019
Content provided by Mayo Clinic ©1998-2026 Mayo Foundation for Medical Education and Research (MFMER). All rights reserved. Terms of Use