Heart transplant
Overview
A heart transplant is an operation in which a diseased, failing heart is replaced with a healthier donor heart. Heart transplant is a treatment that's usually reserved for people whose condition hasn't improved enough with medications or other surgeries.
While a heart transplant is a major operation, your chance of survival is good with appropriate follow-up care.
Why it's done
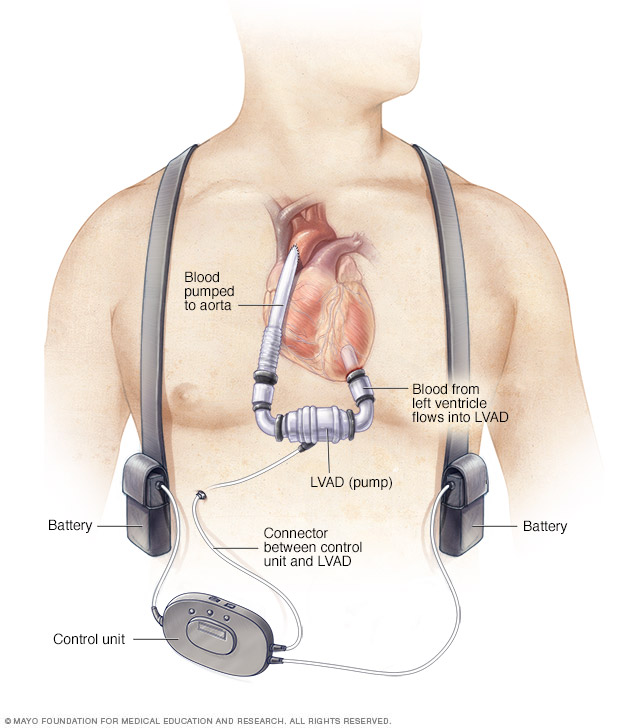
A left ventricular assist device (LVAD) is implanted in your chest. It helps pump blood from the left ventricle of your heart and on to the rest of your body. A control unit and battery pack are worn outside your body and are connected to the LVAD through a port in your skin.
Heart transplants are performed when other treatments for heart problems haven't worked, leading to heart failure. In adults, heart failure can be caused by:
- A weakening of the heart muscle (cardiomyopathy)
- Coronary artery disease
- Heart valve disease
- A heart problem you're born with (congenital heart defect)
- Dangerous recurring abnormal heart rhythms (ventricular arrhythmias) not controlled by other treatments
- Failure of a previous heart transplant
In children, heart failure is most often caused by either a congenital heart defect or cardiomyopathy.
Another organ transplant may be performed at the same time as a heart transplant (multiorgan transplant) in people with certain conditions at select medical centers.
Multiorgan transplants include:
- Heart-kidney transplant. This procedure may be an option for some people with kidney failure in addition to heart failure.
- Heart-liver transplant. This procedure may be an option for people with certain liver and heart conditions.
- Heart-lung transplant. Rarely, doctors may suggest this procedure for some people with severe lung and heart diseases if the conditions cannot be treated with only a heart transplant or a lung transplant.
A heart transplant is not right for everyone, however. You might not be a good candidate for a heart transplant if you:
- Are at an advanced age that would interfere with the ability to recover from transplant surgery
- Have another medical condition that could shorten your life, regardless of receiving a donor heart, such as a serious kidney, liver or lung disease
- Have an active infection
- Have a recent personal medical history of cancer
- Are unwilling or unable to make lifestyle changes necessary to keep your donor heart healthy, such as not drinking alcohol or not smoking
Ventricular assist devices
For some people who cannot have a heart transplant, another option may be a ventricular assist device (VAD). A ventricular assist device is a mechanical pump implanted in your chest that helps pump blood from the lower chambers of your heart (ventricles) to the rest of your body.
VADs are commonly used as temporary treatments for people waiting for heart transplants. These devices are increasingly being used as long-term treatments for people who have heart failure but are not eligible for heart transplants. If a VAD doesn't help your heart, doctors may sometimes consider a total artificial heart — a device that replaces the ventricles of your heart — as an alternative short-term treatment while you're waiting for a heart transplant.
Risks
Besides the risks of having open-heart surgery, which include bleeding, infection and blood clots, risks of a heart transplant include:
-
Rejection of the donor heart. One of the most significant risks after a heart transplant is your body rejecting the donor heart.
Your immune system may see your donor heart as a foreign object and try to reject it, which can damage the heart. Every heart transplant recipient receives medications to prevent rejection (immunosuppressants), and as a result, the rate of rejection continues to decrease. Sometimes, a change in medications will halt rejection if it occurs.
To help prevent rejection, it's critical that you always take your medications as prescribed and keep all your appointments with your doctor.
Rejection often occurs without symptoms. To determine whether your body is rejecting the new heart, you'll have frequent heart biopsies during the first year after your transplant. After that, you won't need biopsies as often.
During the biopsy, a tube is inserted into a vein in your neck or groin and directed to your heart. A biopsy device is run through the tube to take a tiny sample of heart tissue, which is examined in a lab.
- Primary graft failure. With this condition, the most frequent cause of death in the first few months after transplant, the donor heart doesn't function.
- Problems with your arteries. After your transplant, it's possible that the walls of the arteries in your heart could thicken and harden, leading to cardiac allograft vasculopathy. This can make blood circulation through your heart difficult and can cause a heart attack, heart failure, heart arrhythmias or sudden cardiac death.
- Medication side effects. The immunosuppressants you'll need to take for the rest of your life can cause serious kidney damage and other problems.
- Cancer. Immunosuppressants can also increase your risk of developing cancer. Taking these medications can put you at a greater risk of skin and lip tumors and non-Hodgkin's lymphoma, among others.
- Infection. Immunosuppressants decrease your ability to fight infection. Many people who have heart transplants have an infection that requires them to be admitted to the hospital in the first year after their transplant.
How you prepare
Preparations for a heart transplant often begin weeks or months before you receive a donor heart.
Taking the first steps
If your doctor recommends a heart transplant, you'll likely be referred to a heart transplant center for evaluation. Or you can select a transplant center on your own. Check your health insurance to see which transplant centers are covered under your plan.
When evaluating a heart transplant center, consider the number of heart transplants a center performs each year and the survival rates. You can compare transplant center statistics using a database maintained by the Scientific Registry of Transplant Recipients.
You should also check to see if a transplant center offers other services you might need. These include coordinating support groups, assisting with travel arrangements, helping you find local housing for your recovery period or directing you to organizations that can help with these concerns.
Once you decide on a center, you'll need to have an evaluation to see if you're eligible for a transplant. The evaluation will check to see if you:
- Have a heart condition that would benefit from transplantation
- Might benefit from other, less aggressive treatment options
- Are healthy enough to undergo surgery and post-transplant treatments
- Will agree to quit smoking, if you smoke
- Are willing and able to follow the medical program outlined by the transplant team
- Can emotionally handle the wait for a donor heart
- Have a supportive network of family and friends to help you during this stressful time
Waiting for a donor organ
If the transplant center medical team determines that you're a good candidate for a heart transplant, the center will put you on a waiting list. The wait can be long since there are more people who need hearts than donors. Finding a donor depends on your size, your blood type and how sick you are.
While you're on the waiting list, your medical team will monitor your heart and other organs and adjust your treatment as necessary. The team will help you learn to care for your heart by eating well and being active.
If medical therapy fails to support your vital organs as you wait for a donor heart, your doctors might recommend that you have a device implanted to support your heart while you wait for a donor organ. These devices are known as ventricular assist devices (VADs). The devices are also referred to as bridges to transplantation because they gain you some time to wait until a donor heart is available.
Immediately before your transplant surgery
A heart transplant usually needs to occur within four hours of organ removal for the donor organ to remain usable. As a result, hearts are offered first to a transplant center close by and then to centers within certain distances of the donor hospital.
The transplant center will provide you with a pager or cellphone to notify you when a potential heart is available. You must keep your cellphone or pager charged and turned on at all times.
Once you're notified, you and your transplant team have limited time to accept the donation. You'll have to go to the transplant hospital immediately after being notified.
As much as possible, make travel plans ahead of time. Some heart transplant centers provide private air transportation or other travel arrangements. Have a suitcase packed with everything you'll need for your hospital stay, as well as an extra 24-hour supply of your medications.
Once you arrive at the hospital, your doctors and transplant team will conduct a final evaluation to determine if the donor heart is suitable for you and if you're ready for surgery. If your doctors and transplant team decide that either the donor heart or surgery isn't appropriate for you, you might not be able to have the transplant.
What you can expect
During the procedure
Heart transplant surgery is an open-heart procedure that takes several hours. If you've had previous heart surgeries, the surgery is more complicated and will take longer.
You'll receive medication that causes you to sleep (general anesthetic) before the procedure. Your surgeons will connect you to a heart-lung bypass machine to keep oxygen-rich blood flowing throughout your body.
Your surgeon will make an incision in your chest. Your surgeon will separate your chest bone and open your rib cage so that he or she can operate on your heart.
Your surgeon then removes the diseased heart and sews the donor heart into place. He or she then attaches the major blood vessels to the donor heart. The new heart often starts beating when blood flow is restored. Sometimes an electric shock is needed to make the donor heart beat properly.
You'll be given medication to help with pain control after the surgery. You'll also have a ventilator to help you breathe and tubes in your chest to drain fluids from around your lungs and heart. After surgery, you'll also receive fluids and medications through intravenous (IV) tubes.
After the procedure
You'll initially stay in the intensive care unit (ICU) for a few days, then be moved to a regular hospital room. You're likely to remain in the hospital for a week or two. The amount of time spent in the ICU and in the hospital varies from person to person.
After you leave the hospital, your transplant team will monitor you at your outpatient transplant center. Due to the frequency and intensity of the monitoring, many people stay close to the transplant center for the first three months. Afterward, the follow-up visits are less frequent, and it's easier to travel back and forth.
You'll also be monitored for any signs or symptoms of rejection, such as shortness of breath, fever, fatigue, not urinating as much or weight gain. It's important to let your transplant team know if you notice any signs or symptoms of rejection or infection.
To determine whether your body is rejecting the new heart, you'll have frequent heart biopsies in the first few months after heart transplantation, when rejection is most likely to occur. The frequency of necessary biopsies decreases over time.
During a heart biopsy, a doctor inserts a tube into a vein in your neck or groin and directs it to your heart. The doctor runs a biopsy device through the tube to remove a tiny sample of heart tissue, which is examined in a lab.
You'll need to make several long-term adjustments after you have had your heart transplant. These include:
-
Taking immunosuppressants. These medications decrease the activity of your immune system to prevent it from attacking your donated heart. You'll take some of these medications for the rest of your life.
Because immunosuppressants render your body more vulnerable to infection, your doctor might also prescribe antibacterial, antiviral and antifungal medications. Some drugs could worsen — or raise your risk of developing — conditions such as high blood pressure, high cholesterol, cancer or diabetes.
Over time, as the risk of rejection decreases, the doses and number of anti-rejection drugs can be reduced.
-
Managing medications, therapies and a lifelong care plan. After a heart transplant, taking all your medications as your doctor instructs and following a lifelong care plan are vital.
Your doctor might give you instructions regarding your lifestyle, such as wearing sunscreen, not using tobacco products, exercising, eating a healthy diet and being careful to lower your risk of infection.
Follow all of your doctor's instructions, see your doctor regularly for follow-up appointments, and let your doctor know if you have signs or symptoms of complications.
It's a good idea to set up a daily routine for taking your medications so that you don't forget. Keep a list of all your medications with you at all times in case you need emergency medical attention, and tell all your doctors what you take each time you're prescribed a new medicine.
- Cardiac rehabilitation. These programs incorporate exercise and education to help you improve your health and recover after a heart transplant. Cardiac rehabilitation, which you might start before you're released from the hospital, can help you regain your strength and improve your quality of life.
Results
Most people who receive a heart transplant enjoy a good quality of life. Depending on your condition, you may be able to resume many of your daily life activities, such as returning to work, participating in hobbies and sports, and exercising. Discuss with your doctor what activities are appropriate for you.
Some women who have had heart transplants can become pregnant. However, talk to your doctor if you're considering having children after your transplant. You'll likely need medication adjustments before becoming pregnant, as some medications can cause pregnancy complications.
Survival rates after heart transplantation vary based on a number of factors. Survival rates continue to improve despite an increase in older and higher risk heart transplant recipients. Worldwide, the overall survival rate is more than 85% after one year and about 69% after five years for adults.
What if your new heart fails?
Heart transplants aren't successful for everyone. Your new heart can fail for a number of reasons. Your doctor might then recommend adjusting your medications or, in more extreme cases, having another heart transplant.
If additional treatment options are limited, you might choose to stop treatment. Discussions with your heart transplant team, doctor and family should address your expectations and preferences for treatment, emergency care and end-of-life care.
Content Last Updated: November 16, 2019
Content provided by Mayo Clinic ©1998-2026 Mayo Foundation for Medical Education and Research (MFMER). All rights reserved. Terms of Use