C-section
Overview
Cesarean delivery (C-section) is a surgical procedure used to deliver a baby through incisions in the abdomen and uterus.
A C-section might be planned ahead of time if you develop pregnancy complications or you've had a previous C-section and aren't considering a vaginal birth after cesarean (VBAC). Often, however, the need for a first-time C-section doesn't become obvious until labor is underway.
If you're pregnant, knowing what to expect during a C-section — both during the procedure and afterward — can help you prepare.
Why it's done
Sometimes a C-section is safer for you or your baby than is a vaginal delivery. Your health care provider might recommend a C-section if:
- Your labor isn't progressing. Stalled labor is one of the most common reasons for a C-section. Stalled labor might occur if your cervix isn't opening enough despite strong contractions over several hours.
- Your baby is in distress. If your health care provider is concerned about changes in your baby's heartbeat, a C-section might be the best option.
- Your baby or babies are in an abnormal position. A C-section might be the safest way to deliver the baby if his or her feet or buttocks enter the birth canal first (breech) or the baby is positioned side or shoulder first (transverse).
- You're carrying multiples. A C-section might be needed if you're carrying twins and the leading baby is in an abnormal position or if you have triplets or more babies.
- There's a problem with your placenta. If the placenta covers the opening of your cervix (placenta previa), a C-section is recommended for delivery.
- Prolapsed umbilical cord. A C-section might be recommended if a loop of umbilical cord slips through your cervix ahead of your baby.
- You have a health concern. A C-section might be recommended if you have a severe health problem, such as a heart or brain condition. A C-section is also recommended if you have an active genital herpes infection at the time of labor.
- Mechanical obstruction. You might need a C-section if you have a large fibroid obstructing the birth canal, a severely displaced pelvic fracture or your baby has a condition that can cause the head to be unusually large (severe hydrocephalus).
- You've had a previous C-section. Depending on the type of uterine incision and other factors, it's often possible to attempt a VBAC. In some cases, however, your health care provider might recommend a repeat C-section.
Some women request C-sections with their first babies — to avoid labor or the possible complications of vaginal birth or to take advantage of the convenience of a planned delivery. However, this is discouraged if you plan on having several children. Women who have multiple C-sections are at increased risk of placental problems as well as heavy bleeding, which might require surgical removal of the uterus (hysterectomy). If you're considering a planned C-section for your first delivery, work with your health care provider to make the best decision for you and your baby.
Risks
Like other types of major surgery, C-sections also carry risks.
Risks to your baby include:
- Breathing problems. Babies born by scheduled C-section are more likely to develop transient tachypnea — a breathing problem marked by abnormally fast breathing during the first few days after birth.
- Surgical injury. Although rare, accidental nicks to the baby's skin can occur during surgery.
Risks to you include:
- Infection. After a C-section, you might be at risk of developing an infection of the lining of the uterus (endometritis).
- Postpartum hemorrhage. A C-section might cause heavy bleeding during and after delivery.
- Reactions to anesthesia. Adverse reactions to any type of anesthesia are possible.
- Blood clots. A C-section might increase your risk of developing a blood clot inside a deep vein, especially in the legs or pelvic organs (deep vein thrombosis). If a blood clot travels to your lungs and blocks blood flow (pulmonary embolism), the damage can be life-threatening.
- Wound infection. Depending on your risk factors and whether you needed an emergency C-section, you might be at increased risk of an incision infection.
- Surgical injury. Although rare, surgical injuries to the bladder or bowel can occur during a C-section. If there is a surgical injury during your C-section, additional surgery might be needed.
- Increased risks during future pregnancies. After a C-section, you face a higher risk of potentially serious complications in a subsequent pregnancy than you would after a vaginal delivery. The more C-sections you have, the higher your risks of placenta previa and a condition in which the placenta becomes abnormally attached to the wall of the uterus (placenta accreta). The risk of your uterus tearing open along the scar line from a prior C-section (uterine rupture) is also higher if you attempt a VBAC.
How you prepare
If your C-section is scheduled in advance, your health care provider might suggest talking with an anesthesiologist about any possible medical conditions that would increase your risk of anesthesia complications.
Your health care provider might also recommend certain blood tests before your C-section. These tests will provide information about your blood type and your level of hemoglobin, the main component of red blood cells. These details will be helpful to your health care team in the unlikely event that you need a blood transfusion during the C-section.
Even if you're planning a vaginal birth, it's important to prepare for the unexpected. Discuss the possibility of a C-section with your health care provider well before your due date. Ask questions, share your concerns and review the circumstances that might make a C-section the best option. In an emergency, your health care provider might not have time to explain the procedure or answer your questions in detail.
After a C-section, you'll need time to rest and recover. Consider recruiting help ahead of time for the weeks after the birth of your baby.
If you don't plan to deliver any more children, you might talk to your health care provider about long-acting reversible birth control or permanent birth control.
What you can expect
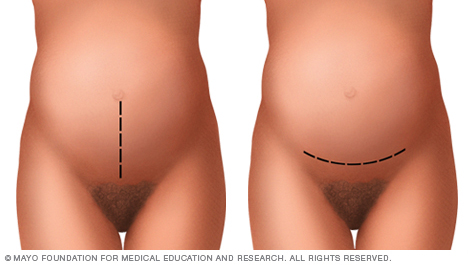
A C-section includes an abdominal incision and a uterine incision. The abdominal incision is made first. It's either a vertical incision between your navel and pubic hair (left) or, more commonly, a horizontal incision lower on your abdomen (right).
Before the procedure
While the process can vary, depending on why the procedure is being done, most C-sections involve these steps:
- At home. Your health care provider might ask you to shower with an antiseptic soap the night before and the morning of your C-section. Don't shave your pubic hair within 24 hours of your C-section. This can increase the risk of a surgical site infection. If your pubic hair needs to be removed, it will be trimmed by the surgical staff just before surgery.
- At the hospital. Your abdomen will be cleansed. A tube (catheter) will likely be placed into your bladder to collect urine. Intravenous (IV) lines will be placed in a vein in your hand or arm to provide fluid and medication.
- Anesthesia. Most C-sections are done under regional anesthesia, which numbs only the lower part of your body — allowing you to remain awake during the procedure. Common choices include a spinal block and an epidural block. In an emergency, general anesthesia is sometimes needed. With general anesthesia, you won't be able to see, feel or hear anything during the birth.
During the procedure
While the process can vary, depending on why the procedure is being done, most C-sections involve these steps:
- At home. Your health care provider might ask you to shower with an antiseptic soap the night before and the morning of your C-section. Don't shave your pubic hair within 24 hours of your C-section. This can increase the risk of a surgical site infection. If your pubic hair needs to be removed, it will be trimmed by the surgical staff just before surgery.
- At the hospital. Your abdomen will be cleansed. A tube (catheter) will likely be placed into your bladder to collect urine. Intravenous (IV) lines will be placed in a vein in your hand or arm to provide fluid and medication.
- Anesthesia. Most C-sections are done under regional anesthesia, which numbs only the lower part of your body — allowing you to remain awake during the procedure. Common choices include a spinal block and an epidural block. In an emergency, general anesthesia is sometimes needed. With general anesthesia, you won't be able to see, feel or hear anything during the birth.
After the procedure
After a C-section, you'll probably stay in the hospital for a few days. Your health care provider will discuss pain relief options with you.
Once the effects of your anesthesia begin to fade, you'll be encouraged to drink plenty of fluids and walk. This helps prevent constipation and deep vein thrombosis. Your health care team will monitor your incision for signs of infection. If you had a bladder catheter, it will likely be removed as soon as possible.
You will be able to start breast-feeding as soon as you feel up to it. Ask your nurse or a lactation consultant to teach you how to position yourself and support your baby so that you're comfortable. Your health care team will select medications for your post-surgical pain with breast-feeding in mind.
Before you leave the hospital, talk with your health care provider about any preventive care you might need. Making sure your vaccinations are current can help protect your health and your baby's health.
When you go home
During the C-section recovery process, discomfort and fatigue are common. To promote healing:
- Take it easy. Rest when possible. Try to keep everything that you and your baby might need within reach. For the first few weeks, avoid lifting anything heavier than your baby. Also, avoid lifting from a squatting position.
- Seek pain relief. To soothe incision soreness, your health care provider might recommend a heating pad, ibuprofen (Advil, Motrin, others), acetaminophen (Tylenol, others) or other medications to relieve pain. Most pain relief medications are safe for women who are breast-feeding.
- Avoid sex. To prevent infection, avoid sex for six weeks after your C-section.
You might also consider not driving until you are able to comfortably apply brakes and twist to check blind spots without the help of pain medication. This might take one to two weeks.
Check your C-section incision for signs of infection. Pay attention to any signs or symptoms you experience. Contact your health care provider if:
- Your incision is red, swollen or leaking discharge
- You have a fever
- You have heavy bleeding
- You have worsening pain
If you experience severe mood swings, loss of appetite, overwhelming fatigue and lack of joy in life shortly after childbirth, you might have postpartum depression. Contact your health care provider if you think you might be depressed, especially if your signs and symptoms don't fade on their own, you have trouble caring for your baby or completing daily tasks, or you have thoughts of harming yourself or your baby.
The American College of Obstetricians and Gynecologists recommends that postpartum care be an ongoing process rather than just a single visit after your delivery. Have contact with your health care provider within the first three weeks after delivery. Within 12 weeks after delivery, see your health care provider for a comprehensive postpartum evaluation. During this appointment your health care provider will check your mood and emotional well-being, discuss contraception and birth spacing, review information about infant care and feeding, talk about your sleep habits and issues related to fatigue and do a physical exam. This might include a check of your abdomen, vagina, cervix and uterus to make sure you're healing well. In some cases, you might have the checkup earlier so that your health care provider can examine your C-section incision. Use this visit to ask questions about your recovery and caring for your baby.
Content Last Updated: June 12, 2020
Content provided by Mayo Clinic ©1998-2026 Mayo Foundation for Medical Education and Research (MFMER). All rights reserved. Terms of Use