Endometrial ablation
Overview
Endometrial ablation is a procedure that surgically destroys (ablates) the lining of your uterus (endometrium). The goal of endometrial ablation is to reduce menstrual flow. In some women, menstrual flow may stop completely.
No incisions are needed for endometrial ablation. Your doctor inserts slender tools through the passageway between your vagina and uterus (cervix).
The tools vary, depending on the method used to ablate the endometrium. Methods might include extreme cold, heated fluids, microwave energy or high-energy radiofrequencies.
Some types of endometrial ablation can be done in your doctor's office. Others must be performed in an operating room. Factors such as the size and condition of your uterus will help determine which endometrial ablation method is most appropriate.
Why it's done
Endometrial ablation is a treatment for excessive menstrual blood loss. Your doctor might recommend endometrial ablation if you have:
- Unusually heavy periods, sometimes defined as soaking a pad or tampon every two hours or less
- Bleeding that lasts longer than eight days
- Anemia from excessive blood loss
To reduce menstrual bleeding, doctors generally start by prescribing medications or an intrauterine device (IUD). Endometrial ablation might be an option if these other treatments don't help or if you're not able to have other therapies.
Endometrial ablation generally isn't recommended for postmenopausal women or women who have:
- Certain abnormalities of the uterus
- Cancer of the uterus, or an increased risk of uterine cancer
- An active pelvic infection
Risks
Complications of endometrial ablation are rare and can include:
- Pain, bleeding or infection
- Heat or cold damage to nearby organs
- A puncture injury of the uterine wall from surgical instruments
Future fertility
Pregnancy can occur after endometrial ablation. However, these pregnancies might be higher risk to mother and baby. The pregnancy might end in miscarriage because the lining of the uterus has been damaged, or the pregnancy might occur in the fallopian tubes or cervix instead of the uterus (ectopic pregnancy).
Some types of sterilization procedures can be done at the time of endometrial ablation. If you are having endometrial ablation, long-lasting contraception or sterilization is recommended to prevent pregnancy.
How you prepare
In the weeks before the procedure, your doctor might:
- Perform a pregnancy check. Endometrial ablation can't be done if you're pregnant.
- Check for cancer. A thin tube (catheter) is inserted through your cervix to obtain a small sample of your endometrium to be tested for cancer.
- Remove an IUD. Endometrial ablation isn't performed with an IUD in place.
- Thin your endometrium. Some types of endometrial ablation are more successful when the uterine lining is thin. Your doctor might prescribe medications or perform a dilation and curettage (D&C), a procedure in which the doctor scrapes out the extra tissue.
- Discuss anesthesia options. Some methods of endometrial ablation require general anesthesia, so you're asleep during the procedure. Other types of endometrial ablation might be performed with conscious sedation or with numbing shots into your cervix and uterus.
What you can expect
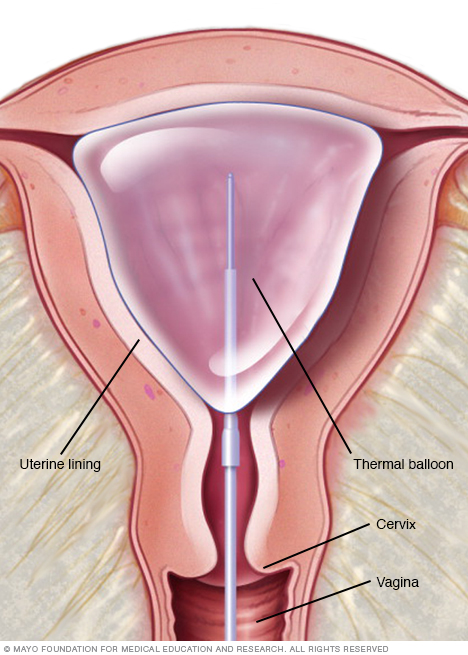
One type of endometrial ablation uses a thermal balloon filled with heated fluid to destroy the lining of the uterus (endometrium).
During the procedure
Endometrial ablation can be performed in your doctor's office. But some types of endometrial ablation are performed in a hospital, especially if you will need general anesthesia.
The opening in your cervix needs to be widened (dilated) to allow for the passage of the instruments used in endometrial ablation. Dilation of your cervix can happen with medication or the insertion of a series of rods that gradually increase in diameter.
Endometrial ablation procedures vary by the method used to remove or destroy the endometrium. Options include:
- Electrosurgery. A slender scope is used to see inside the uterus. An instrument passed through the scope, such as a wire loop, is heated and used to carve furrows into the endometrium. Electrosurgery requires general anesthesia.
- Cryoablation. Extreme cold is used to create two or three ice balls that freeze and destroy the endometrium. Real-time ultrasound allows the doctor to track the progress of the ice balls. Each freeze cycle takes up to six minutes, and the number of cycles needed depends on the size and shape of your uterus.
- Free-flowing hot fluid. Heated saline fluid is circulated within the uterus for about 10 minutes. An advantage of this method is that it can be performed in women who have an irregular-shaped uterus from abnormal tissue growth — such as intracavity lesions or uterine fibroids — that distorts the uterus.
- Heated balloon. A balloon device is inserted through your cervix and then inflated with heated fluid. Depending on the type of balloon device, the procedure can take from two to 10 minutes.
- Microwave. A slender wand is inserted through the cervix. The wand emits microwaves, which heat the endometrial tissue. Treatment usually lasts three to five minutes.
- Radiofrequency. A special instrument unfurls a flexible ablation device inside the uterus. The device transmits radiofrequency energy that vaporizes the endometrial tissue in one to two minutes. The device is then removed from the uterus.
After the procedure
After endometrial ablation, you might experience:
- Cramps. You may have menstrual-like cramps for a few days. Over-the-counter medications such as ibuprofen or acetaminophen can help relieve cramping.
- Vaginal discharge. A watery discharge, mixed with blood, may occur for a few weeks. The discharge is typically heaviest for the first few days after the procedure.
- Frequent urination. You may need to pass urine more often during the first 24 hours after endometrial ablation.
Results
It might take a few months to see the final results, but endometrial ablation usually reduces the amount of blood lost during menstruation. Most women will have lighter periods, and some will stop having periods entirely.
Endometrial ablation isn't a sterilization procedure, so you should continue to use contraception. Pregnancy might still be possible, but it will likely be hazardous and end in miscarriage.
Content Last Updated: November 20, 2020
Content provided by Mayo Clinic ©1998-2026 Mayo Foundation for Medical Education and Research (MFMER). All rights reserved. Terms of Use